Matula Thoughts
Oct 5, 2018
October incongruities & congruities.
3813 words

One.
October is an odd month, not just with its odd number of days and shortening hours of daylight, but with unpredictable weather shifts including tropical cyclones, the Atlantic hurricanes and Pacific typhoons. Autumn is already in progress and Michigan is fortunate to witness spectacular foliage displays that peak this later this month. October lacks much in the way of major national holidays. Columbus Day, October 8 this year, is observed variably, in some states, Puerto Rico, banks, school districts, the Postal Service, federal and state agencies, but not generalized nationally or celebrated at Michigan Medicine.
Columbus Day had its start when the Tammany Society in NYC and the Massachusetts Historical Society in 1792 celebrated the 300th anniversary of the Columbus landing. A century later, President Benjamin Harrison similarly highlighted the 400th anniversary. Harrison, notably, was the only president (so far) who was the grandson of a president. Columbus Day became a state-level holiday in Colorado in 1907, in 1934 Franklin Roosevelt designated October 12 a national holiday, and since 1971 it has been set on the second Monday of October. The ambiguous details of European “discovery” of America, problematic from the indigenous people perspective, makes it unlikely that Columbus Day will have a long future as a national holiday. Alternatively, Hawaii celebrates Discoverer’s Day and Vermont declared it Indigenous Peoples’ Day. Native American Day is celebrated by California and Nevada on the fourth Friday of September, while in South Dakota on October’s second Monday. Tennessee observes American Indian Day on the fourth Monday of September and other countries in the Americas have their own origin celebrations.
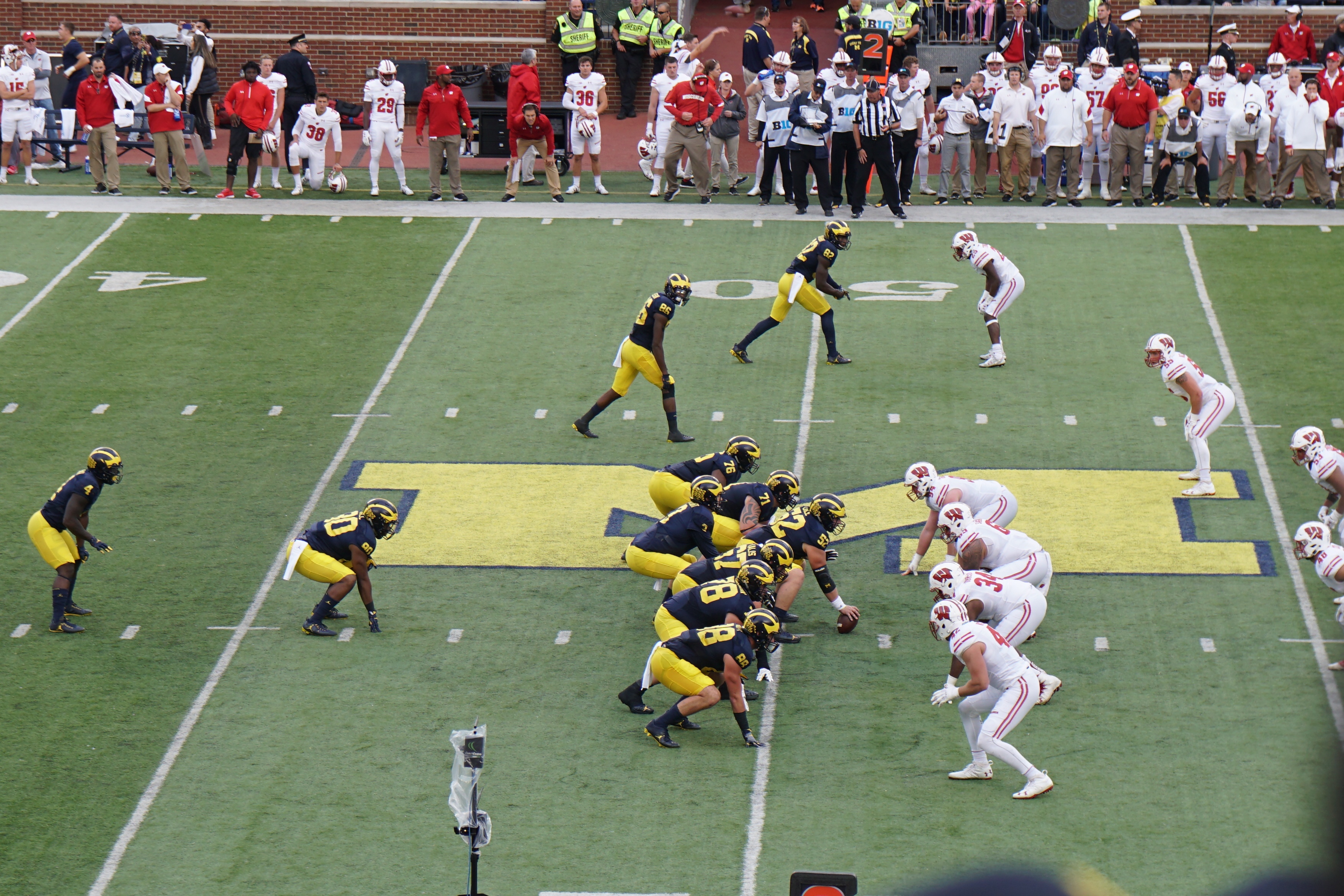
University homecoming events provide other respites in October, although our Urology Department held its Nesbit Alumni reunion prematurely last month, nearly colliding with our biennial Dow Health Services Research Symposium due to coordination with autumn scientific meetings, religious holidays, and the dominating effect of the home football schedule relegating the 2018 Nesbit Meeting to September’s Nebraska game.
October ends with Halloween, an ancient Celtic harvest tradition, now centered on costumed children prowling their neighborhoods for treats, ostensibly as bribes to withhold pranks. Carved pumpkins or turnips become jack-o’-lanterns signaling target-rich households. Pumpkins are more octagonal than spherical to my eye and Halloween face-carving liberates pumpkin fruit for pies and pepita snacks. [Above: Irish Halloween turnip lantern, Museum of Country Life, Turlough Village, County Mayo, Ireland. Courtesy, Wikipedia. Below: October 2, 2018, Dee Fenner and Red Maple tree, outside Dean’s wing.]

Two.

Recollections of last month include the opening of Michigan Medicine’s Brighton Specialty Center, a large organizational effort led by John Wei, yielding 300,000 square feet of new clinical space. Anne Cameron did three of the first cases in the Brighton Center for Specialty Care operating rooms. [Above: John Wei at pre-opening ceremony. Below: Anne & OR team September 24.]

Our Dow Health Services Research Symposium #4, directed by Chad Ellimoottil and Lindsey Herrel, featured TED-style talks at Power Center.


[Above: Matt Nielsen University of North Carolina with slide congratulating Lindsey and Chad. Below: Greg Auffenberg (Nesbit 2017), Brent Hollenbeck, Chris Saigal of UCLA, Jim Montie.]

The featured speakers and short abstracts and lightning presentations were first rate, including Preeti Malani and Ken Warner (below).

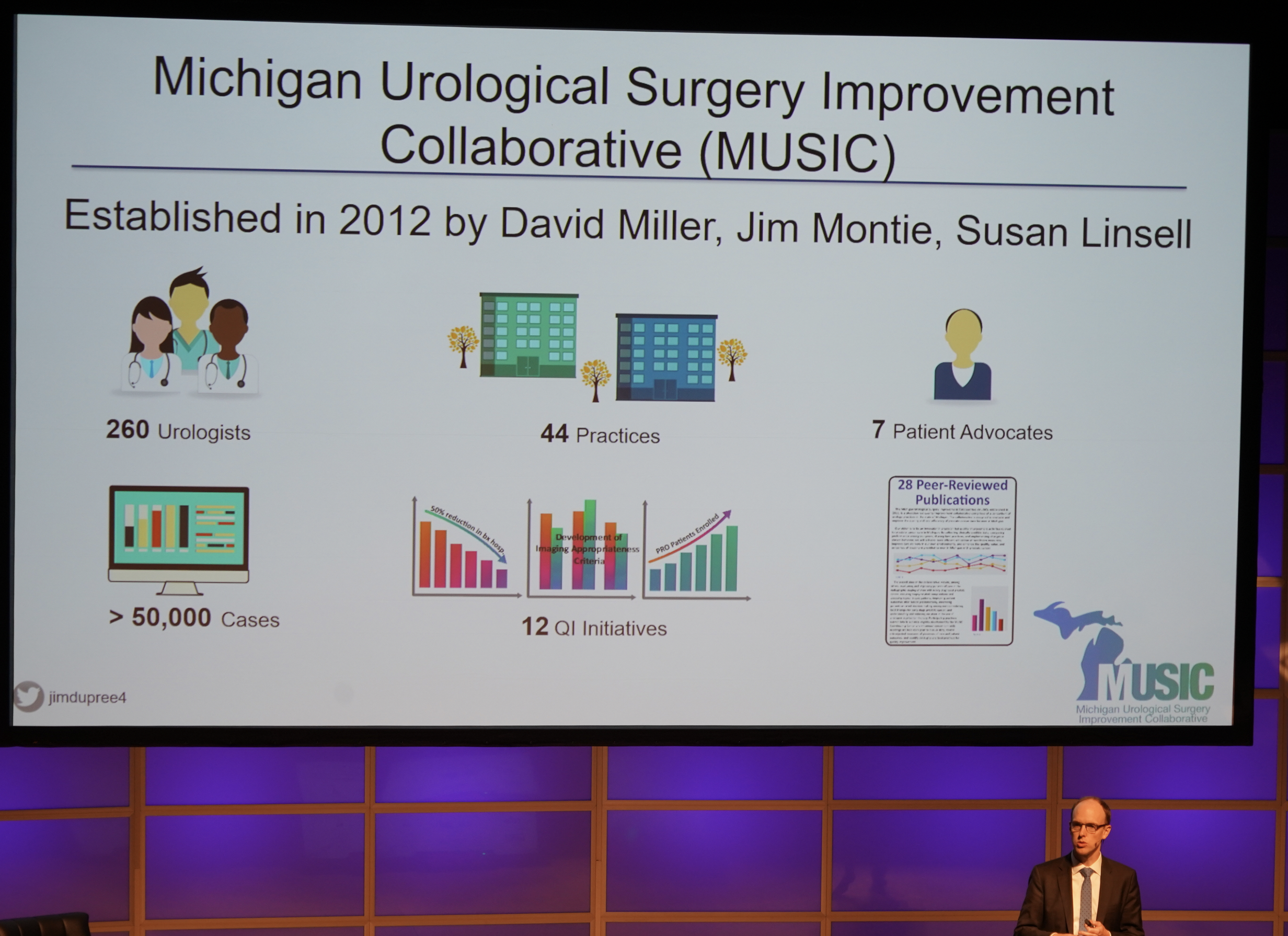
The flying microphone, shown below with Rod Dunn, livened up the atmosphere. Jim Dupree discussed the successful Michigan Urological Surgical Improvement Collaborative (also below).

The following week Chris Sweeney, of Harvard Medical School/Dana Farber Cancer Institute, gave the Jerry Weisbach Lecture, speaking on clinical trial insights regarding prostate cancer heterogeneity. [Below: Chris & Ganesh Palapattu.]


The Nesbit Reunion, later in the week at NCRC (above), featured Toby Chai, Professor of Urology at Yale (Nesbit 1994) as Nesbit visiting professor who gave two excellent talks.


Our own Matt Davenport was the Nesbit guest speaker. John Wei did a superb job, as Secretary-Treasurer, organizing the program and event. [Above: Toby & Matt. Below: John Wei & Sherman Silber N’73.]

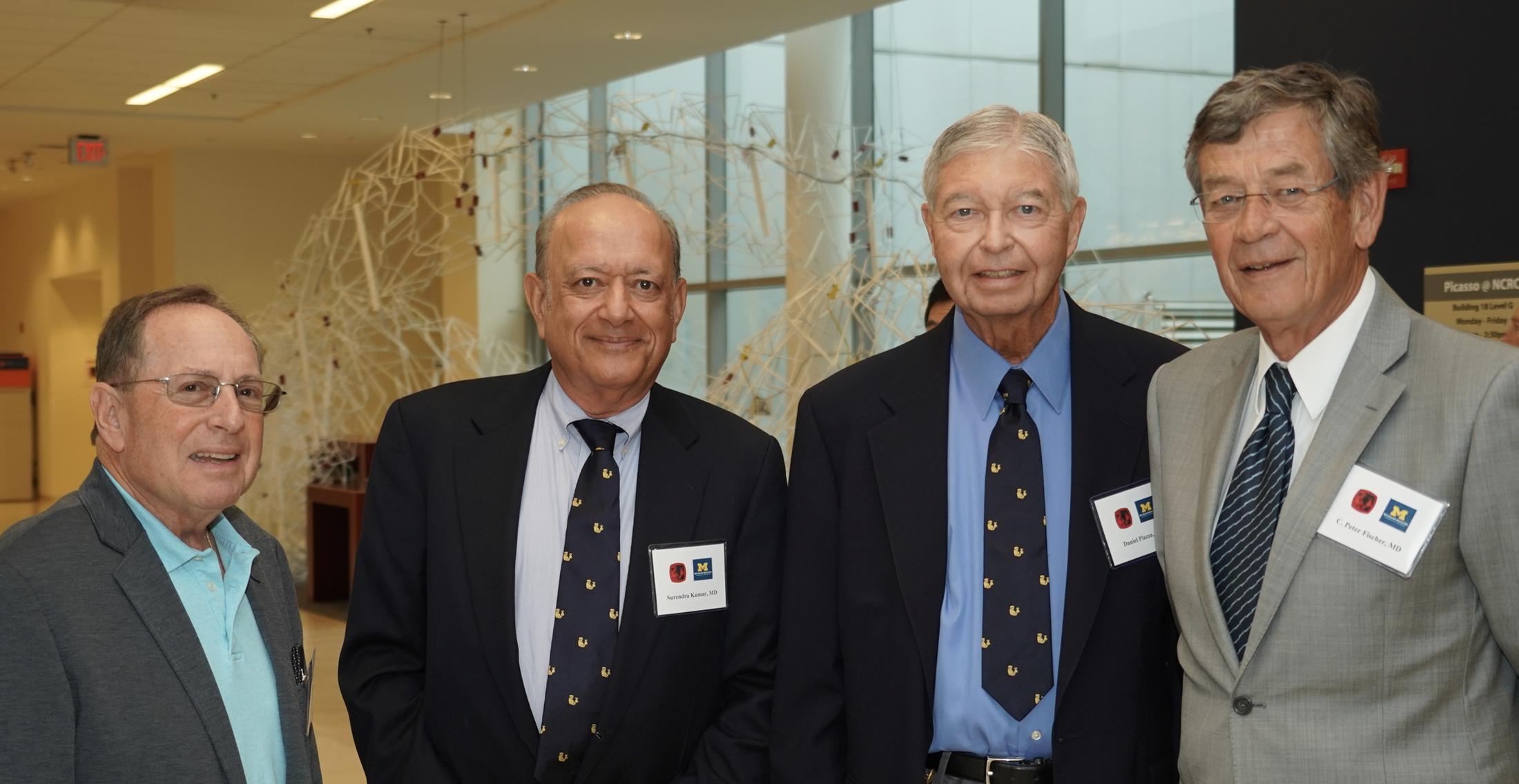
Sherman Silber spoke on “Progress making sperm and eggs from skin.” We also heard Kevin Stone and Brian Stork from West Shore Urology. [Below: Dave Harrold N’1978, Surendra Kumar N’81, Dan Piazza N’79, C. Peter Fischer N’79.]
[Below: Utah Pete Fisher N’06 & son Mitch.]

The Nesbit Tailgate entertained alumni and friends from around the country and the victory over Nebraska completed the weekend. Next year, around this time, we will launch the Centennial of Urology at Michigan. [Below top: Meidee Goh, sister Lindee from Boston, husband David Fry; bottom: Yuting Fan, Sherman Silber, David Burk N’89 & brother-in-law Rupert Baily from North Carolina.]


Next year’s Nesbit Reunion, 2019, will open up the year-long Michigan Urology Centennial.
Three.

Octopus, octagon, octogenarian, and October come from the Proto-European h₁oḱtṓw stem for eight, an odd fact given that this is the tenth calendar month of the year. How this came to be is a curious quirk of calendar history.

Lunar phases provided the first “calendars” throughout most of human history, marking time between solar days and solar years using the moon’s regular phases. Lunar phases are still essential for fishermen and sailors to predict tides, noting big swings in tidal amplitude during full and new moons (spring tides) and lesser differences during the quarter phases (neap tides). Etruscans and Romans approximated 8-day weeks to lunar cycles to coordinate commercial markets, political affairs, and holidays, although some fudging was necessary each year to match the solar cycle. An early Roman calendar ran from March through December with lunar cycles that filled up 304 days, exclusive of 51 winter days during an “unorganized expanse” of slack time. [Wikipedia entry Nundinae.] The ten calendar months of Romulus were then: Martius, Aprilis, Maius, Iunius, Quintilis, Sextilis, September, October, November, and December.
Julius Caesar gave us the Julian calendar, bringing Roman calendar years into closer agreement with solar years. He implemented the new system on January first in a year that he had no way of knowing would be 45 BC. The Julian Calendar offered three normal years with 365 days and an intervening leap year of 366 days, to make up for the inexact match of solar days to solar years. The leap day was doubled every fourth year to maintain solar synchrony, but nevertheless the calendar gradually lost its alignment with the solar year and by the time of Pope Gregory XIII in 1582, the asynchrony had drifted to 10 full days. Lawyer and law teacher in his earlier career, Ugo Boncompagni was summoned to Rome by Pope Paul III and served Paul IV and Paul V before election to Pope himself. His term was one of church reform, largely in response to the Protestant Reformation. [Below: Pope Gregory XIII portrait by Lavinia Fontana in list of extant papal tombs. Wikipedia.]

Gregory XIII refined the Julian Calendar by advancing the calendar that year so that 4 October was followed, the next day, by 15 October and using leap year spacing to make the average year 365.2425 days long. The Gregorian Calendar, fixing the 10-day drift and shortening the average year by 0.0075 days, is widely used throughout the world today for business and government. Because of Gregory XIII, the October of 1582 lacked a 5th day and nine others in between. The credit for the math involved belongs to Aloysius Lilius, an Italian physician and astronomer, and Christopher Clavius, a German Jesuit astronomer and mathematician.
Science has proven the actual length of solar days vary, due to tides sloshing around and slowing rotation of the Earth. The solar year (tropical year) in 2000 was 365.24219 ephemeris days, ephemeris time (ET) being defined by orbital period rather than axial rotation of Earth. The Système International (SI) divides an ephemeris day into 86,200 SI seconds. For most landlubbers lunar phases have limited utility, although they still show up on modern wrist watches, that keep us on time.

Four.

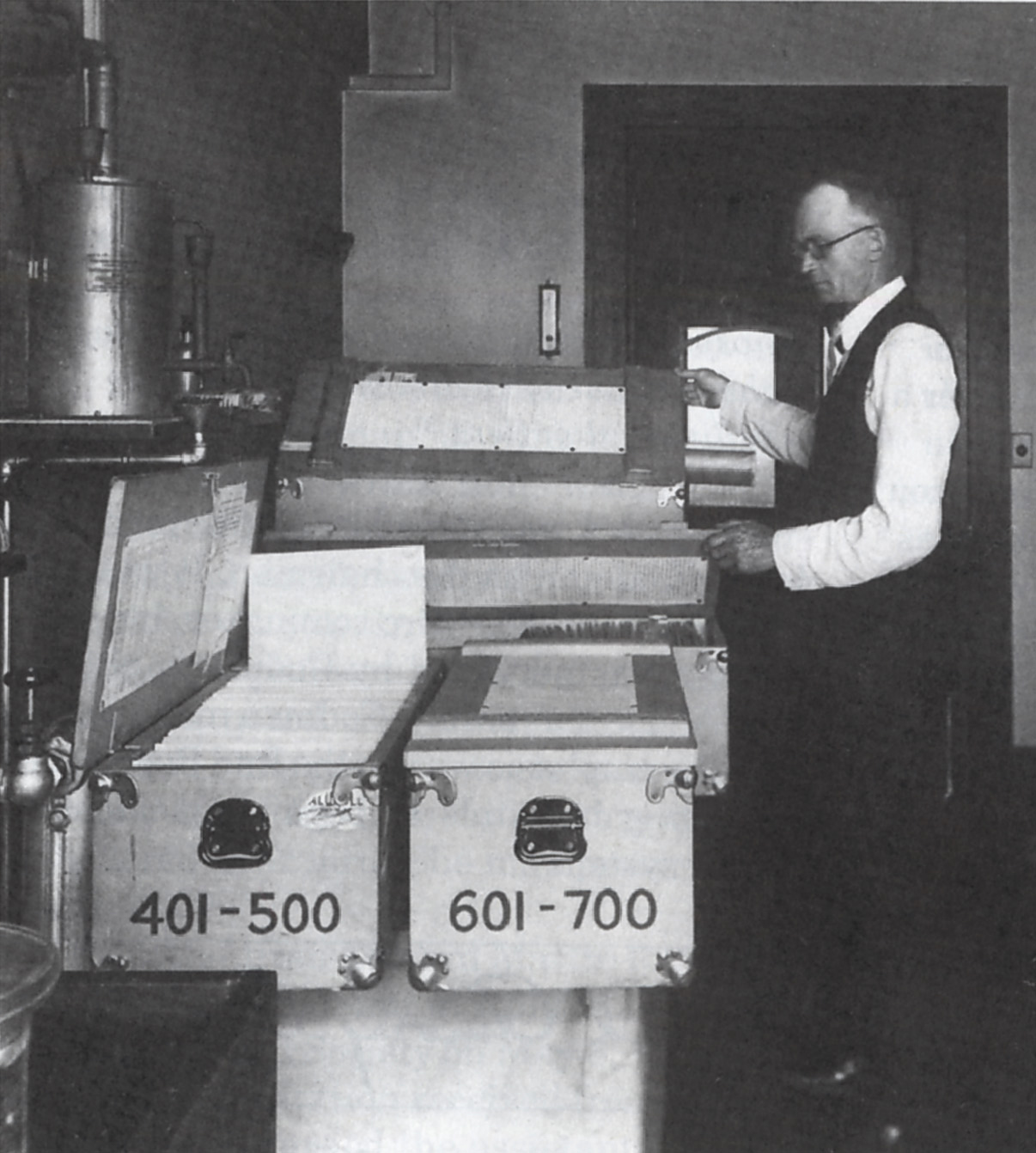
The regular weekly focal point of our department is 7 AM Thursday, regardless of month, when residents and faculty assemble for conferences where each summer a tide of 4th year medical students begins as rotating “clinical clerks” begin to audition for residency training slots. Students spend a month with us in clinics, hospital rounds, operating rooms, and then make individual presentations at Grand Rounds, having been directed and mentored by residents, fellows, and faculty. The tide recedes when nationwide formal interviews begin in October. [Above: Thursday 7 AM conference.]
Out of around 340 students who apply, around 20 clinical clerks, and 47 who interview, we will match 4 students who will spend their next five years or more with us. The candidate pool is very strong academically and in terms of individual personalities, life experiences, drive, and talents, these students are the best of the best of medical students. The proof is seen in our residents.
It is a tough time to be a medical student and entering medicine. Most students have accumulated egregious debt in the form of student loans. This fact is a black mark on our society. There is little excuse for a large medical school tuition bill, students create enough personal debt with living expenses alone during medical school. Society, particularly that of advanced industrialized nations, can afford to teach its next generation of health care workers. As it is, young doctors spend large fractions of their income paying back their debt (with interest) to banks and other funding sources – money that they would otherwise pump back into the economy through local stores, car dealers, home purchases, and Amazon. Philanthropy too would be served because former trainees in their first years of practice would be more likely each year to give a hundred bucks or so to the institutions that taught them (and even to the Nesbit Society), thus developing “a habit of giving back” rather than trying to stay afloat in the tsunami of educational debt.
The uncertainty of health care economics adds to the difficulty for students, and massive regulatory changes coming from the federal government place academic medicine and all of health care at risk, perhaps the greatest risk in our time. Yet, all times have been tough, and many of the best and brightest people continue to choose medical careers.
Five.
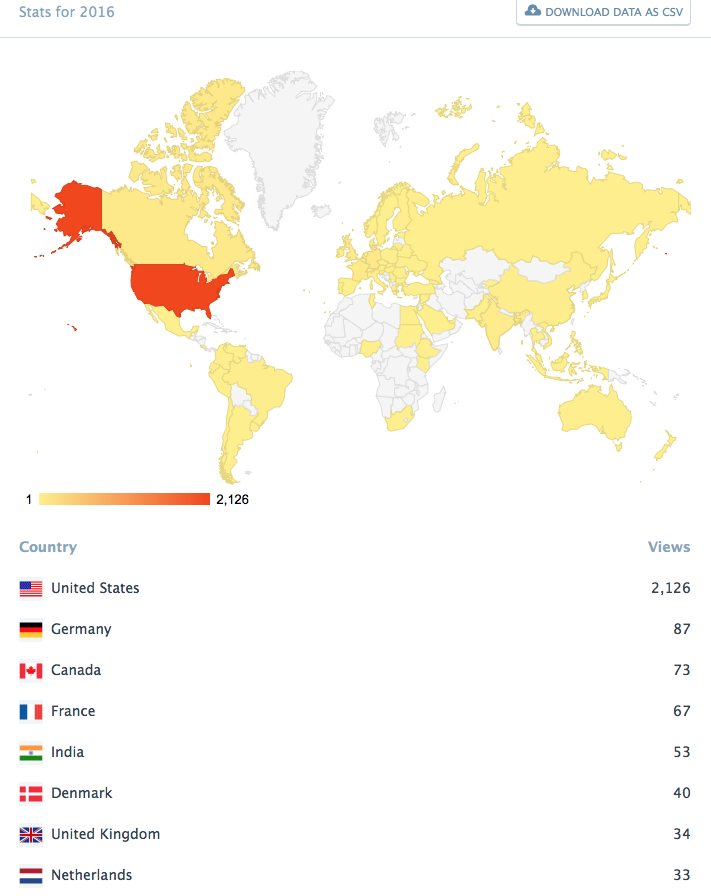
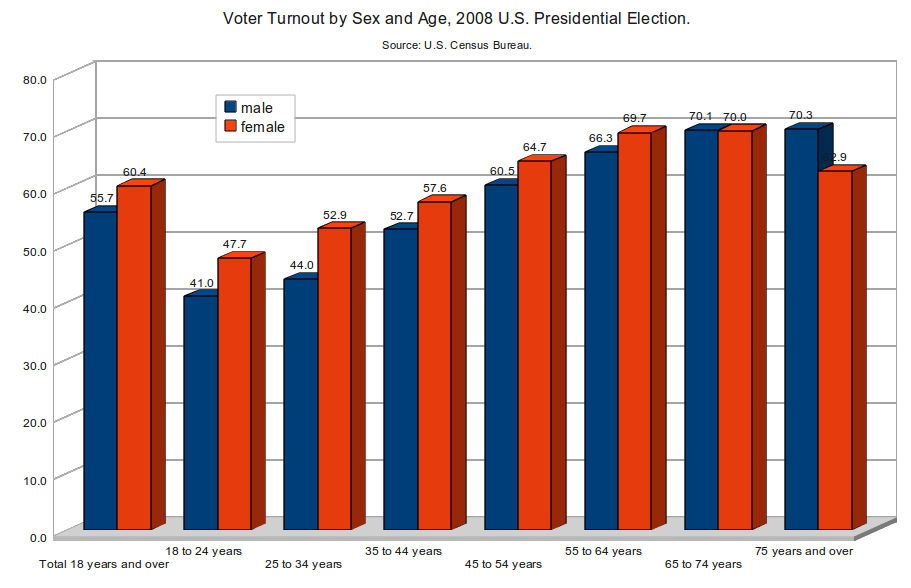
Political campaigning heats up in October with elections next month for governor, state legislators, other regional officers, one third of the US Senate, and the US House of Representatives. Voter turnout in the US tends to be around 58% of eligible voters in national presidential election and 40% in mid-term elections. Even less turn out in odd years, primaries, or local elections, indicating that Americans take the responsibility of democracy far too lightly. This fact should disturb us at least as much as the idea of foreign governments messing with our processes (that’s what rough opponents do – so why are we surprised and apparently so defenseless?) Below is a chart from the U.S. Census Bureau.
Our predecessors worked hard and against odds to create a government of the people, by the people, and for the people. The Declaration of Independence is a beautiful and aspirational document that explains why people should be entrusted to their own destiny, The Constitution creates a working framework for government, and its Bill of Rights presents a list of individual protections from authority (with some nonsense that politics mixed into it). A greater cynic might argue, given the voter turnout data, that today’s citizens are not working hard enough to protect foundational elements of western society.
On the other hand, deception has its moments and admits many self-serving hucksters and bad actors to the corridors of power. Voters are often attracted to bright shiny celebrities, single issue extremists, or deceptive campaigns. Trickery is part of the human confection, one classic example being the Trojan Horse of Homer’s stories, although new technologies magnify the possibilities of deception and crowd manipulation. Technology aside, our society has failed to properly educate an informed citizenry capable of critical thinking. Biologic trickery takes many forms, and the octopus is one of the most versatile masters, using camouflage, mimicry, threat, shape-shifting, and environmental opacification. While octopi (scientific order Octopoda) may be the biologic champions, humans are good learners.

[Jens Petersen. Image of greater blue-ringed octopus, Hapalochlaena lunulata. Tasik Ria, North Sulawesi, Indonesia GFDL license. Wikipedia.]
Six.
Octoberfest. Beer and political campaigning mingle in October. Octoberfest, as a celebration, dates back to 12 October 1810, when citizens of Munich attended festivities around the royal marriage of King Ludwig I to Princess Therese. Münchners, Munich’s community-folk, gathered peacefully to drink beer, watch horse races, and enjoy a day off work, unless they were helping with the crowd, distributing the food and beer, or organizing the races. Civilization requires organizers, workers, and leaders.
Octoberfest has spread around the world as a respite from routine of work and a chance to celebrate as a community. For some people this is simply an excuse to drink beer, but others enjoy some civic sensibility. Beer and other spirits may help navigate the politics that necessarily attend all communities and the periodic stress of politicking to elect around 500,000 state and national public officials.
Leadership is an unfortunate necessity of human affairs, and over the course of documented history it is evident that most leadership has been self-serving, foolish, and extended the sum total of human misery. Nevertheless, seven billion humans need forms of leadership to organize sports, workplaces, community events, local governments, geographic regions, religions, and nations.
The U.S. Congress on 23 January, 1845 passed “An act to establish a uniform time for holding elections of President and Vice President in all the States of the Union.” The Tuesday after the first Monday of November was selected and that date continues to this time. Federal elections occur only in even-numbered years, and presidential elections take place every four years. October, the heaviest month of campaigning, is exhilarating for many people as evidence of the aspiration of “government of the people, by the people, and for the people.” Election day is a public holiday in some states and territories, but not Michigan. November 5 is our next election day.
Seven.
October fiction. October Country, the name of a 1943 Ray Bradbury collection of stories, conveys a sense of the oddness of October. The introductory “mini-story,” The Grim Reaper, in the modern paperback version, is a stark commentary on modern humankind in the mid-20th century. [Bradbury. The October Country. Del Rey Ballantine Books, NY. 1996.]
Bradbury used the title, The October Country, as a metaphor for that time of the year when people and places become melancholy with thoughts and preparations for winter. His dystopian novel, Fahrenheit 451, imagines the dark winter of an authoritarian society where free speech no longer exists. The 1966 Francis Truffaut film version with Julie Christie was a classic in its own right. Bradbury (1920-2012), along with Isaac Asimov, Arthur Clark, Robert Heinlein, and Stanislaw Lem carried science fiction into the literary mainstream according to a 2012 obituary [Gerald Jonas, NYT, June 6, 2012.]:
“The futuristic world envisioned by Bradbury among others is coming fast upon us, compelled by the erosion of democracy and the ascendency of technology. We not be able to curtail the latter, but we should be shamed by our pathetic efforts as a species to build and disperse democratic institutions and human rights.”
Machine-learning algorithms, even those multi-layer “neural” networks capable of “deep learning,” in my opinion can ever equate to human intelligence. Programs and systems are built by people susceptible to particular ideologies, biases, “isms,” greed, and other intoxications that plague everyone and their clever systems invariable reflect some, but not all particularities. These algorithms are already in play in our lives and will become increasingly pervasive with autonomous capabilities in many sectors of our lives, however we must be cautious of accepting artificial intelligence (AI) as a substitute for human authenticity. How can AI distinguish between fact and true facts, given the mutability of fact and truth and their continual arbitration, in “real time,” by human values, science, and consensus? A cynic might argue that AI shouldn’t be expected to distinguish between facts and true facts if most humans can’t do so.
Ian Fleming’s final James Bond book, the 14th in the series, Octopussy and the Living Daylights, was a collection of short stories published posthumously in 1966, originally with just those two stories, but later including The Property of a Lady and also 007 in New York. The first story and provided the backstory for the film Octopussy, with Roger Moore in 1983. A pet octopus, owned by the villain, give that story its name and elements of the other stories found their way into other Bond films.
Eight.
October tides. Back in the times of the earliest wine and beermakers, days were defined by sunrises and sunsets, tides and lunar phases framed the weeks, and sun and star positions marked out months and years. It must have taken a leap of faith for early thinkers to convince themselves that something as far away as the moon could physically move the massive oceans of earth, but the tidal relationships to moon and sun were recognized as early as the second century BC by Hellenistic astronomer Seleucus of Seleucia who linked tides to lunar position, with height of tides depending on the position of the moon relative to the sun.
Tide tables were made for tourists in China in 1056 so that they could coordinate visits to the legendary tidal bore of the Qiantang River. Due to the mismatch in size between the Hangzhou Bay and Qiantang (Tsientang) River, this daily occurrence with 30 foot tides moving at 25 mph, can double in size when the moon and coincidental typhoons align. This has been celebrated for thousands of years during the 8th month of the lunar year, known as the Mid-Autumn Festival. [David K. Lynch. Scientific American. January, 1982. Alan Taylor. The Atlantic. Sept. 20, 2016.]
Newton may have been deemed a tidal bore when wrote the essay Discourse on the Tides, in 1616 in a letter to Cardinal Orsini and later used calculations and his theory of universal gravitation in Principia in 1687 to explain the tidal influences of sun and moon. Great Lakes tides at their greatest reach 5 centimeters, although much larger standing waves called seiches, caused by wind and atmospheric pressure, are mistaken for tides.
Nine.
Tecumseh, Harrison, and the Battle of the Thames. The Thames River in Ontario comes to mind in relation to a famous Native American who died on this day, October 5, 1813. We have many referrals for patient care from our neighboring town, Tecumseh, and while I vaguely recognized this as a Native American name, I knew little until I looked it up and learned this day is the anniversary of a battle in 1813 when Chief Tecumseh was killed at the age of 45. An American Shawnee, he was born in Ohio Country and he grew up amidst the American Revolution and the Northwest Indian Wars. He became a great leader, compelling orator, and staunch advocate for tribal unity.
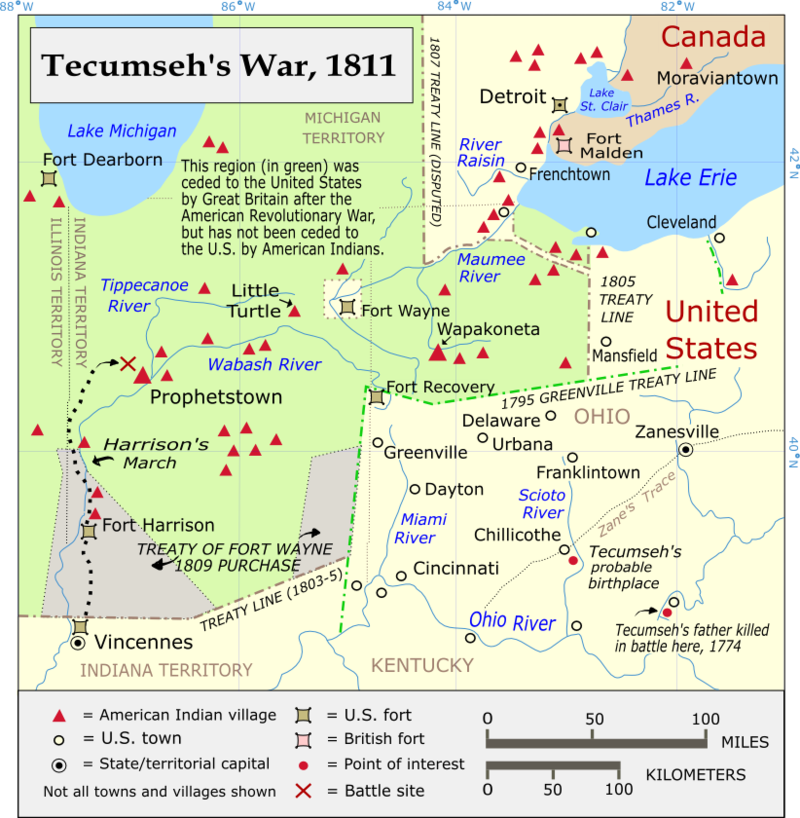
Tecumseh’s War in Indiana Territory between his American Indian confederacy and the U.S. began with a confrontation in 1810 at Grouseland, the home of William Henry Harrison, governor of the territory. Conflict continued with a defeat for the multi-tribal confederacy at the Battle of Tippecanoe in 1811, and spilled over into the War of 1812 after Tecumseh formed an alliance with Great Britain that helped capture Fort Detroit. After the fledgling U.S. Navy gained control of Lake Erie in 1813, the British and multi-tribal confederacy retreated into Canada, where American Forces engaged them at the Battle of the Thames (also known as the Battle of Moraviantown) and Tecumseh was killed.
[Above: Tecumseh, attrib. Owen Staples. Toronto Public Library. Below: Tecumseh’s War map by Kevin Myers, Wikipedia.]
[Below: Battle of Tippecanoe. Alonzo Chappel Collection, Smithsonian Institute.]

With the death of Tecumseh, the confederacy collapsed and Detroit returned to American control, where only four years later the University of Michigan would be established. Most native Americans were eventually pushed west of the Mississippi.
Harrison considered Tecumseh remarkable, once calling him a genius. With soaring popularity after the War of 1812 Harrison became U.S. House Representative in 1816 and Senator in 1825, truncated by appointment as Minister Plenipotentiary to Gran Columbia in 1828. He returned to private life in Ohio at his farm, but was prompted to make a few runs for presidency, ultimately winning and becoming ninth American President in 1841, the last president born before the Revolution.
Harrison’s term was short-lived as Harrison was sworn in on 4 March 1841 and died of pneumonia a month later. Vice President John Tyler assumed office, but a constitutional crisis concerning succession lingered for more than a century until resolution by the Twenty-fifth Amendment of 1967. Tyler was the son of Founding Father Benjamin Harrison V and the paternal grandfather of 23rd U.S. President Benjamin Harrison, who nationalized Columbus Day.
It might be argued that the choice of our ninth president was a risky one from the point of health vulnerability, at age 68 he was the oldest sworn into office until Ronald Reagan in 1981 at 69. On the other hand, far younger presidents and major political leaders have been cut short by disease or assassination, so perhaps age should be a minor consideration for long range leadership. Representative democracy seems a far better method of leadership selection than royalty, birthright, or sectarian succession, but genetics (or epigenetics) always seems to be lurking behind the scenes as the American presidency has shown through Adams, Harrison, Roosevelt, and Bush.
Ten.
Octopus traps and Halloween spiders. Matula Thoughts often seeks threads or themes, sometimes risking belaboring a point or putting too fine an edge on a detail, such as comparing pumpkins to octagons, or relating October to medicine. Of course, October 16, 1846 was the first demonstration of general anesthesia.
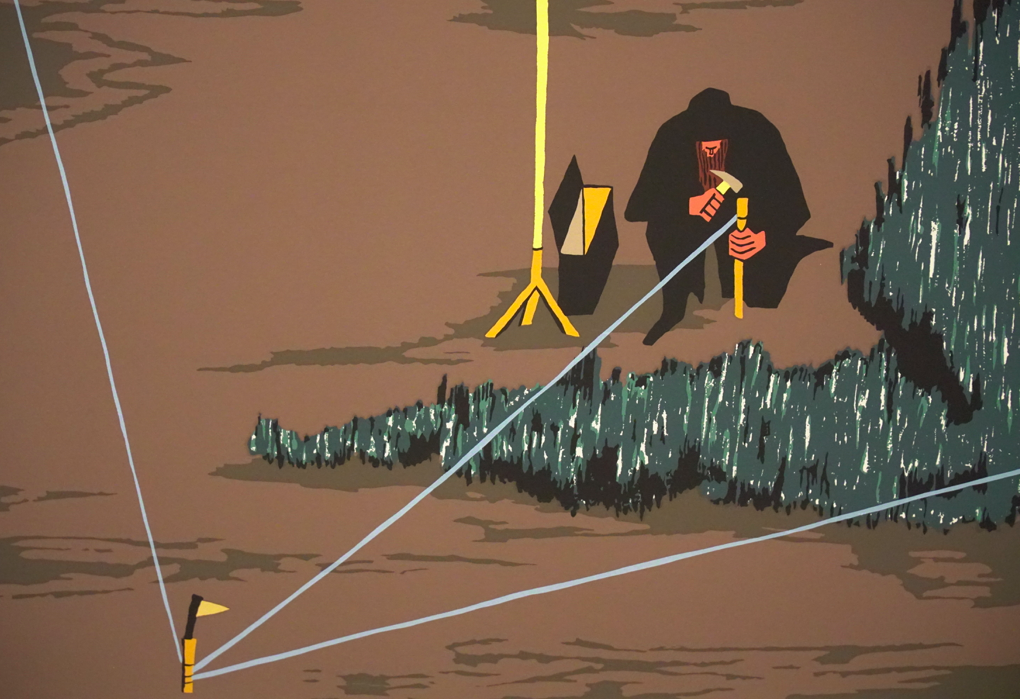
A stretch to the octo stem brings in Takotsubo cardiomyopathy, a non-ischemic heart crisis of sudden temporary weakening of the muscle also known as stress cardiomyopathy, transient apical ballooning cardiomyopathy, or the broken heart syndrome, and leading to acute heart failure, lethal ventricular arrhythmias, or ventricular rupture. Most cases (85%) are set in motion by severe physical or emotional distress that causes myofibrillar degeneration. The first studied case was by Sabo et al in Japan, reported in 1991, and the name came from the traditional octopus traps used by Japanese fishermen, setting them out when the tides were favorable. [Yoshihiro YJ, Goldstein DS, Barbaro G, Ueyama T. Takotsubo cardiomyopathy. Circulation. 118:2754, 2008.] [Below: octopus traps, Wikipedia, public domain.]

Octopi aside, eight doesn’t have a heavy presence in biology, Stedman’s Dictionary expends barely a half a page to words beginning with oct. Although spiders and ticks (larger category = class, Arachnida) have eight legs, octo hasn’t tainted their names. Spiders rank seventh in species diversity among all organisms, with nearly 90,000 species compared to 300 species of octopi, and our single human species. Spiders (biologic classification order, Araneae) have enormously complex genomics and have a universal ability to make silks and venoms. [Pennisi. Science. 358:288, 2018.] Spiders scare kids and are completely congruous with Halloween, so be prepared with shock, awe, and a basket of treats when permutations of 8-legged creatures knock at your door at the end of this month. [Below: Marvel Spider-Man symbiote suit.]

Thanks for reading Matula Thoughts.
David A. Bloom
University of Michigan, Department of Urology, Ann Arbor
![]()