
DAB What’s New Oct 7, 2016
Education, errors, & box scores
3931 words
One. Autumn is academic medicine’s high season. With summer officially over the serious work is well underway for faculty promotions, graduate medical education (GME) in academic centers, and continuing medical education in professional meetings. Residency interviews are beginning. Coincidentally, this is also the definitive season for baseball as major league teams compete for its World Series. [Above: San Francisco Giants 6 – St. Louis Cardinals 2. Sept 15, 2016. Cueto pitching.]
With participants notching up their games, rookie mistakes become occasional, although errors never totally go away. Performance measurements allow individuals to understand and improve their work, while inviting inevitable comparisons. Fielders in baseball, for example, are judged by errors: the number of times they fail to complete plays that could have been made by common effort, a term roughly equivalent to the reasonable and standard practice by which physicians are judged.

[Derek Jeter, Yankee shortstop. 8/24/08. Photographer Keith Allison]
It may seem awkward for physicians to talk of mistakes, however these conversations are not only necessary, but also healthy when done properly. We formalize these conversations in morbidity and mortality (M&M) conferences. Fortunately, most errors are minor if not trivial and are intrinsic to all biologic behaviors, indeed species variation itself is built on error. Health care cannot be expected to be exempt from error, for who among us has not missed a blood draw or an IV placement on first puncture? Who has not made a transcription error when typing an entry into today’s electronic medical record systems. (When I trained to become a surgeon, typing skills were not a required skill set; today many surgeons spend nearly as much time typing as operating – surely an epic waste of health care resources.) On the other hand, serious complications such as postoperative bleeding, deep venous thromboses, anastomotic leaks, or missed relevant comorbidities, bear inspections that should inspire personal and systemic improvements to minimize errors for future patients. While we take errors very seriously, we can’t let them disable us, for the next patient is always in line.
The point to make is that the conversation of error in health care is essential. The practice of medicine is, indeed, a practice and things that don’t turn out as intended need to be investigated to improve quality of practice. Charles Bosk’s 1979 book, Forgive and Remember, is a classic starting point. You can get a good summary of it in Robin Williamson’s review of its 2003 edition [J. Royal Society of Medicine. 2004 Mar; 97(3): 147-148]. While surgical fields have a long history of tough treatment of trainees, surgical training today (GME) is far less recriminating when errors are the result of earnest effort. [Below: Ed McGuire lecturing as emeritus professor to residents last year.]

Two. An astonishing array of events emblematic of our three-way mission initiated the 2016 academic high season of urology in Ann Arbor.
Inspiring Discovery was a celebration at North Campus Research Center focusing on partnerships with donors that fuel education and research. Tom Varbedian, distinguished Michigan alumnus, friend of our department, and retired ophthalmologist was among those honored, in his instance for support of medical students. He has funded 14 students over the years and 4 “Varbedian scholars” are presently here in medical school. [Below: Tom and some of his students]

The evening was rich in meaningful stories of partnerships between donors and faculty to grow the conceptual basis and technology of health care while educating the next generation. Endowments are the key strength of Michigan’s future as a great academic medical center.
Dow Division Health Services Research Symposium targeted the topic of performance. The program by Jim Dupree, Khurshid Ghani, and Chad Ellimoottil featured our own and other world-wide experts who investigate and innovate health care delivery. This third biennial meeting included around 200 attendees.

Jerry Weisbach Lectureship last month brought Martin Gleave from Vancouver, BC to discuss his extraordinary work co-targeting the androgen receptor and adaptive survival pathways in advanced prostate cancer.
Nesbit alumni weekend featured Freddie Hamdy from Oxford University describing his unique randomized trial of active monitoring, radical prostatectomy, and radiotherapy for localized prostate cancer. Two NEJM papers from his group last month attracted international attention and Freddie’s talk to us was the first public presentation. At the cutting edge of reproductive medicine, Sherman Silber explained how the Y-chromosome is becoming redundant in the light of the incredible accomplishment of creating sperm and ova from skin fibroblasts. Many other talks filled the program. We were honored to have senior urologists Cheng-Yang Chang, Clair Cox, and Mark McQuiggan in the audience. Cheryl Lee (Chair at OSU) and Stu Wolf (Associate Dean at Austin’s Dell SOM) were honored at our alumni dinner and John Park won the John Konnak award for service to our department. A lively Nesbit tailgate party preceded the Wisconsin football game.

[Above: Freddie Hamdy presents results of prostate cancer trial. Below: Freddie Hamdy, Marschall Runge, Sherman Silber, Jim Monte & Nesbit attendees]

After the Nesbit tailgate we saw Michigan edge Wisconsin out 14-7. Next year’s Nesbit alumni reunion will align with the Air Force Academy game here in Ann Arbor.

[Clair & Clarice Cox tailgating]
The Montie Visiting Professor was Ian Thompson, Jr., Director of the Cancer Therapy & Research Center of the University of Texas in San Antonio. Ian (below) spent childhood years (1956-59) in Ann Arbor when his father was on the Michigan urology faculty. A West Point graduate, Ian became Colonel in the U.S. Army and chair of urology at University of Texas San Antonio. He is President of the American Board of Urology. He spoke to us on the future of prostate cancer detection and therapy, and heard superb presentations from our residents and fellows.

[Ian Thompson, Jim Montie]
This past month has been rich in education. Although these costly events interrupt the clinical work that supplies their main funding, they are educationally essential and important for quality improvement and team alignment. Quality of care is improved by expanding the conceptual basis of medical practice, clinical skills and professionalism of the workforce, and delivery systems. Alignment of healthcare workers is critical to their success in teams. In the face of new technology, new diseases, and a changing socio-economic-political environment these educational efforts cannot be sacrificed to clinical throughput.
Three. The attendant at the gas station of life was a picturesque metaphor of Dr. Horace Davenport as he taught first year physiology to medical students here in Ann Arbor in the later 20th century (re-quoted by us in July What’s New and Matula Thoughts). The actuality of a physician’s role is more complex, as Dr. Davenport well knew, and the irony of his specific term attendant in the midst of an academic medical center full of attendings was probably intentional. (Another irony is that today’s gas stations, in contrast to those of Davenport’s time, are mostly self-service).
A physician is better understood from the neuroscience perspective with respect to mirror neurons. Humans are not unique in having these sophisticated forms of quorum sensors that facilitate empathy, a phenomenon seen in certain other biologic species such as crows, elephants, and of course fellow primates. Humans, however, have tools, skills, and systems that allow highly developed ways to operationalize empathy.
Physicians can no longer speak so territorially about their roles because health care is provided as significantly by nurses, physician assistants, and other advanced practice providers (APPs). The awkward term health care provider has crept into general use, and while downplaying the physician as a professional, the new terminology is necessary in the team play of modern healthcare. Regulatory and corporate forces reduce health care services to commodity encounters that match diagnostic codes to treatment codes. Many encounters can be delegated to APPs working at high ends of their scopes of practice. While vaccinations, dental cleaning, and sports physicals can readily be commoditized, whether routine “well patient” check ups or visits for uncharacterized problems can be similarly commoditized in 15 to 30-minute encounters remains to be seen. Some patients need the magic of attention and intuition from a health care professional that is not readily translated to check lists or passed down the ladder of expertise.
Effective attendants at life’s service stations hone their skills to observe and listen carefully while practicing their craft. In the process of listening and observing they need not only determine a patient’s diagnosis and an attendant treatment (ICD 10 and corresponding CPT codes), but also must discover relevant issues of the context of that person’s life in terms of livelihood, family, neighborhood, or socioeconomic condition. Context amplifies or minimizes any diagnosis and therapy. Without understanding the patient’s life story, that is the ultimate co-morbidities, an actual encounter in the office may have little value to the patient. All this is to say that effective attendants (physician, medical assistant, nurse, advanced practice provider, etc.) must seek to understand the patient as fully as possible, although such understanding is illusive and always incomplete.
Four. Rabbit holes in time. An article earlier this year in The Lancet by Kingshuk Pal, “Could you wait a second,” described a clinic visit with a woman in her mid-thirties. The encounter was allocated for a mere 10 minutes in his National Health Service (NHS) clinic in London, and in spite of an earlier add-on patient Pal was back on time for the last patient of the morning. He assumed the visit would be a simple encounter for a prescription, and indeed things started out that way. In fact, Pal had seen the same lady in brief encounters twice before and his colleagues had seen her other times as well to write prescriptions after going through standardized template checklists. However, Pal noted:
“But things didn’t feel quite right. I interrupted my internal monologue to go back over what she had just said … There was something about the vehemence with which she had expressed herself that jarred.”
Follow-up questions led into a “rabbit hole” that revealed an unexpected terrible social situation of an abusive marriage. Pal called in appropriate support services and eventually the lady became able to take control of her life. The missed opportunities to uncover the critical social comorbidity (spousal abuse) that was the basis of all of the previous encounters with the well-intended NHS physicians surely would be considered errors in other occupations. Pal commented on earlier missed opportunities to rescue the patient:
“… each time we had stuck to our templates. We were focused on her medical needs. We had listened to what she said, but not what she meant. What had been left unsaid was how much she needed kindness, sympathy, and patience. For me to give her a few seconds of my silence so that she could finally break hers. I know if I had been busy, it would have seemed like that would take forever. But the passage of time is a peculiar thing. As strange as in a consultation as it is in Wonderland:
Alice: ‘How long is forever?’
White Rabbit: ‘Sometimes, just one second.” [The Lancet. 387:1900-1901, 2016]
Five. Attending at the station. John Berger’s factual description of a rural English general practitioner in the 1960s is an understated gem of medical literature. Berger and photographer Jean Mohr spent six weeks with the doctor. More than shadowing him, they embedded in his practice, living with him and his wife in St. Briavels in the Forest of Dean, Gloucestershire. The physician, John Eskell, was named John Sassall for the book, A Fortunate Man: The Story of a Country Doctor, although accounts of patients and the community were otherwise factual. Berger and Mohr observed Eskell/Sassall in his clinic (called the surgery) and dispensary, as well as on his house calls.
This somber book has underlying themes of optimism in human kindness, meaning, and extraordinary curiosity that some people, such as Eskell possess. Berger explains how the morbidity and comorbidities of patients became the personal burden of Eskell.
“I said that the price which Sassall pays for the achievement of his somewhat special position is that he has to face more nakedly than many other doctors the suffering of his patients and the sense of his own inadequacy. I want now to examine his sense of inadequacy.
There are occasions when any doctor may feel helpless: faced with a tragic incurable disease; faced with obstinacy and prejudice maintaining the very condition which has created the illness or unhappiness; faced with certain housing conditions; faced with poverty.
On most occasions Sassall is better placed than the average. He cannot cure the incurable. But because of his comparative intimacy with patients, and because the relations of a patient are also likely to be his patients, he is well-placed to challenge family obstinacy and prejudice. Likewise, because of the hegemony he enjoys within his district, his views tend to carry weight with housing committees, national assistance officers, etc. He can intercede for his patients on both a personal and bureaucratic level.”
Six. Personalized medicine. Comorbidities unquestionably impact illness, and without understanding them in at least some depth, physicians can hardly claim to deal out meaningful advice and therapy. Today we confuse recognition of comorbidities, by our ability to list billing codes, with actual understanding of comorbidity relevance and impact. Prominent in Sassall’s example is the matter of who he is outside the clinic and dispensary. He represents something positive in the community and accordingly he is not quite free to live a life that doesn’t impact favorably on him, his environment, or his profession. He accepted that “trade-off” when he accepted his role as a physician. Berger continues his explanation.
“He is probably more aware of making mistakes in diagnosis and treatment than most doctors. This is not because he makes more mistakes, but because he counts as mistakes what many doctors would – perhaps justifiably – call unfortunate complications. However, to balance such self-criticism he has the satisfaction of his reputation which brings him ‘difficult’ cases from far outside his own area. He suffers the doubts and enjoys the reputation of a professional idealist.
Yet his sense of inadequacy does not arise from this – although it may sometimes be prompted by an exaggerated sense of failure concerning a particular case. His sense of inadequacy is larger than the professional.
Do his patients deserve the lives they lead, or do they deserve better? Are they what they could be or are they suffering continual diminution? Do they ever have the opportunity to develop the potentialities which he has observed in them at certain moments? Are there not some who secretly wish to live in a sense that is impossible given the conditions of their actual lives? And facing this impossibility do they not then secretly wish to die?” [Berger. A Fortunate Man. 1967. Vintage International Edition 1997. p. 132-133.]
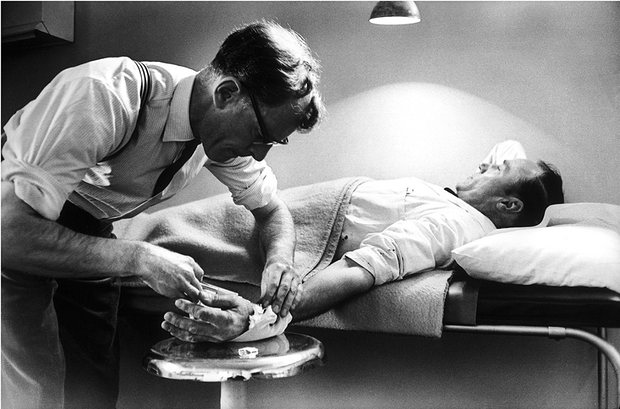
[Jean Mohr photo p. 50]
The doctor confronts existential issues in these questions. Berger makes the case that Sassall’s biggest inadequacy was an inability to counter the comorbidities that framed the immediate morbidities of his patients. Sassall was an idealist who tried to fix morbidities and co-morbidities patient by patient. His intermittent successes fueled his perseverance.
Seven. Mistakes. Medical practice in Eskell’s day was mainly the binary proposition of doctor and patient, family “comorbidity” notwithstanding. Physicians had far fewer tools at their disposal than today’s incredible armamentarium, but it requires teams to deploy modern healthcare’s tools. No single John Eskell can deliver today’s miracles, although confoundingly the complex paradigm of multidisciplinary team medicine greatly increases the opportunities for error. The complexity of healthcare today and the multiplicity of people involved in the teams delivering it, has magnified the chance for mistakes in the intervening half century.
The Journal of the American Medical Association recently introduced a new department, JAMA Professionalism, with an inaugural article on disclosure of medical error. The case summary described a dermatologist who had just performed skin biopsies on two patients only to discover that the instruments he had just used had not been sterilized. The ensuing discussion revolved around the issues of disclosure and analysis of the error to preclude its repetition. [W. Levinson, J. Yeung, S. Ginsburg. Disclosure of medical error. JAMA 316(7):764-765, 2016]
A phrase has stuck with me from John Shook, the insightful “zen-master” of lean processes: I can’t remember exactly where or when he said it, but it goes like this: for us to fulfill our role, we have to keep on learning. 
[John Shook on right with Jack Billi]
Eight. Retrograde thoughts. Everyone brings a unique identity to their work, and in health care the idiosyncrasies of each practitioner resonate with particular specificity in the nature of his or her practice. The professional motivations, world-view, aspirations, distractions, personal demons, work-ethic, curiosity, consistency, empathy, attention to detail, ability to listen and observe, as well as commitment to community are unique to each practitioner and are manifested distinctly in each practice, and with each patient. A mandate for professionalism is intended to bind all these variables together in the practice of medicine, but this is necessarily a vague aspiration although a national trend seeks to define a professional standard and perhaps reduce it to metrics and benchmarks. A national set of professionalism standards or a GME curricular competency can never replace the role models of John Sassall/Eskell and so many others.
It may be subversive to suggest, in today’s world of measurement and precision in medicine, that if you can’t measure something of importance, you still can (and must) improve it. The discovery of what matters to a patient may not be readily measureable. On the other hand, for things that are measureable a certain degree of precision does not matter. Whether you weigh 170 pounds vs. 169.573 pounds, or whether your creatinine is 1.2 or 1.18746, or if your BP is 120/80 or 117.3/78.4 the precision is irrelevant. However, if your abdominal aortic aneurysm or renal transplant are managed by medications that you are reluctant to admit you can’t afford – that fact really matters.
Nine. A growing body of literature punctures any remaining illusions of the perfection of medical practice. Atul Gawande’s Complications and Henry Marsh’s Do No Harm are good examples of this genre of story-telling and introspection. This type of work is instructive, although limited to single examples of individuals, sometimes approaching the point of titillation or voyeurism. Anecdotes certainly have value, acting like fables that accrue in our minds and bring us to greater wisdom in future actions. Lacking any real-time peer review and team-based process improvement, however, these personal denouements and anecdotes are unlikely to achieve larger scale in medical practice quality improvement.
Autopsy of errors or failures is more purposeful in driving deliberate changes in the ways we deploy work, whether in the structure of a clinic visit or the steps in an operative procedure. This turns out to be the very holistic idea of the Toyota Process Systems that has translated in western business as lean engineering. Reconsidering that pseudo-scientific phrase, if you can’t measure it you can’t understand or fix it – this adage is useful, but should not become dogma. Of course, measurement is essential to understanding and improving things, but measurement is not central to all sophisticated human processes. Ideas are central to understanding and progress, and measurement is only a tool used along the way to test hypotheses, measure performances, or test results.
Henry Chadwick (1824-1908) initiated the practice of recording statistics based on his experience in the game of cricket. He applied these methods to baseball after discovering the game in 1856 while “cricket reporter” for the New York Times. His box score for reporting the game, adapted from the cricket box score, has blossomed into contemporary baseball statistics of batting average, runs scored, base on balls, strike outs, runs batted in, earned run average, fielding percentage, and errors, to name a few before falling into the more complex Sabermetrics. Numbers can replicate or model a game, but they cannot substitute for the performance of the game itself.
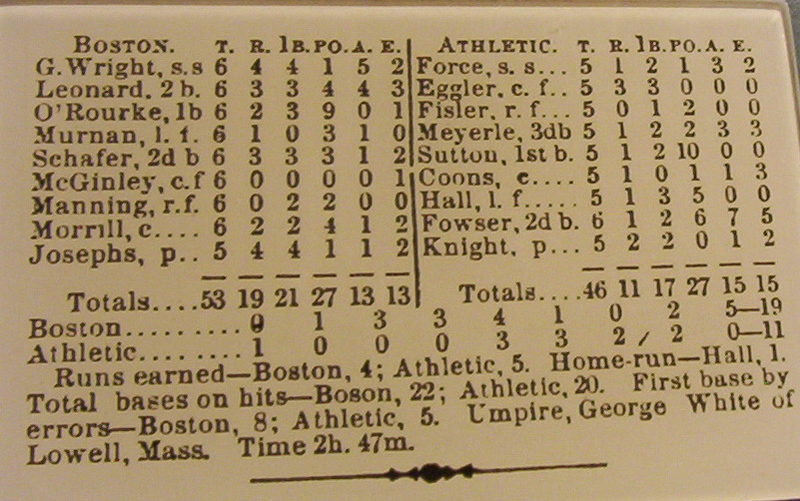
[1876 Box score: Wikipedia]
Ten. Boston surgeon Ernest Amory Codman (1869-1940) was an intellectual successor to Chadwick in the realm of health care, where scoring is more complex than in baseball. [Below: Codman collecting data.]
Eskell and Codman were obsessively committed to their work, but centered on the patient in different ways. Both men were mavericks. Codman focused on measureable outcome, he called this the end result idea, and believed that individual physicians and hospital record systems should keep relevant information. Eskell attended to the patient in the moment and in the environment. Each physician was overwhelmed by his own idea. Codman became alienated from his colleagues and went bankrupt self-publishing his book on the end-result idea, A Study in Hospital Efficiency. Eskell focused on his immediate performance delivering health care one patient at a time, attentive to their inevitable comorbidities, but he ultimately committed suicide. Whether their unfortunate ends were due to highly sensitive mirror neurons overwhelmed by the woes of the world, or obsessive personalities that closed the door to sufficient joy to offset their burdens is a mystery.
The word detachment caught my attention when I finished surgical residency at UCLA. My inspirational chief was William P. Longmire, Jr. and, just as our completing residents and fellows and the Nesbit Society, I was given a diploma when I finished training. The Longmire Society logo was a symbol with four corners that read: Detachment, Method, Thoroughness, and Humility. At the time (it was 1977) I understood three of the attributes, but found detachment somewhat odd: why include that word?
Over the years. I’ve come to understand it better. Clearly, Codman and Eskell suffered from inadequate detachment. Dr. Longmire, a great surgeon, found the right balance. He knew his patients quite well, but had the necessary detachment to make a grand incision, put his hands in the abdomen, and fix most any problem with exquisite skill and judgment. He felt the need to warn young trainees to develop similar detachment.
The world is different today. Minimally invasive surgery, OR checklists, and electronic health records serve their purposes, but distance us from patients. Indeed, with robots a surgeon never needs to physically touch a patient, surrogates and checklists can stand in the way. Don’t get me wrong, I have benefitted from the robot and I believe in systems (although not obsessively). However, when it is not the surgeon’s hand that makes the incision and it’s not the surgeon’s hands in the body, the doctor-patient relationship is changed, even if in a subtle way. This is reminiscent of the old farmer’s adage: if you have ham and eggs for breakfast, the chicken was involved, but the pig was committed. The new tools, the regulations, scorekeeping, and the economics of health care have created an environment of significant detachment for our trainees. We no longer need to warn them to develop that sense, rather we need to inspire the right extent of involvement and commitment that will lead them into rabbit holes and other avenues of inquiry as caring attendants at the gas stations of life.
Health care performance is now judged by a multitude of variables, some worthy and others less so: patient outcomes may not be evident for years, peer review at M & M conferences drives quality improvement, and performance measures du jour, such as Press Ganey data, remind us of our public responsibility. Ultimately, our game has no final box score. The practice of medicine is an individual art, evolving as knowledge and technology accrue and as self-knowledge notches up, one hopes in lockstep with experience, patient by patient, whether in the springtime or autumn of our careers. Measurements can improve elements of our performances, but will never substitute for artful performance itself.
[Michigan 14 – Wisconsin 7, Nesbit Weekend 2016]
David A. Bloom
University of Michigan, Department of Urology, Ann Arbor
