
Matula Thoughts 1 May 2020
2430 words
Back on the road to contagious hospitals
“Reading gives us someplace to go when we have to stay where we are.”
Mason Cooley, American aphorist, 1927-2002.

[UH & UMMS Early spring 2020 on the road from old AA train station to main campus of Michigan Medicine.]
One.
Back on the road. May is usually a sweet spot in the calendar, but not so sweet around the world this year. Some random mistakes in the RNA sequences of a single common virus created a new version that has wrecked worldwide havoc on health, hospitals, and economies. Normally in May, memories and anticipations run strong, for it is a particularly sensual time of the year when colors, smells, tastes, sounds, seem to have especially bright notes after winter dormancy has lifted in the northern hemisphere. That sense of memory and anticipation is reflected in William Carlos Williams’s curious piece, Spring and All [By the road to the contagious hospital], written by the New Jersey physician and published in 1923. The title has long intrigued me and the content continues to puzzle me. Williams was a doctor in New Jersey, who wrote in his spare time. He was an excellent physician, my friend Joan Chiaviello Flanigan recalls from his care for her family when she was a child.
The odd free verse poem of Williams is deliberately mal-organized into 27 sections (identified by Roman enumeration I through XXVII, minus the missing number VII), with random prose interludes of commentary, “chapters,” and unidentified “footnotes” interspersed throughout it. An upside-down Chapter XIII follows a normally-oriented Chapter 19 in the unspecified introduction to the poem. Most verbal images precede spring and are neither attractive or cheering. Spring and All, both poem and its world, is very much upside down and disordered, until XXII and the Red Wheel Barrow that helps set things right. [Below: the confusing “Chapter XIII.”]
Little did we expect, just a year ago writing here about Williams, that we would actually be back on the road to contagious hospitals this May in 2020. Luckily, the Michigan Medicine field hospital at the athletic complex did not require deployment several weeks ago because social distancing and personal hygiene flattened our covid19 curve enough to preclude the new contagious hospital in Ann Arbor – at least for now. Given the widely disseminated knowledge of historians and scientists, it is incredible that we were surprised (again) by a terrible infectious pandemic.
Two.
Contagious diseases worried the University of Michigan Medical School in 1897 when it converted a small laundry shack behind the Homeopathic Hospital into a Contagious Ward for diphtheria, smallpox, and scarlet fever, diseases barely mentioned in medical schools today. In 1914 the city of Ann Arbor, still recalling a 1908 smallpox epidemic, gave the university $25,000 for a new Contagious Disease Hospital with 24-beds in an isolated area, well to the east of the larger hospital grouping. The civic contribution was as much a matter of self-protection than generous philanthropy, although the two attitudes are not unrelated, for philanthropy after all is a self-protective attribute of humanity at the species level. [Below: Michigan’s Contagious Hospital 100 years ago. Bentley Library.]

Williams wrote Spring and All [By the road to the contagious hospital] at an exuberant time for the University of Michigan and its Medical School. Urologist Hugh Cabot, recently appointed dean (in 1921), was building a great medical faculty and new hospital. Michigan’s contagious hospital of that time is now long gone and the idea of contagious hospitals had all but disappeared in Ann Arbor and around the world, until this past winter. Some modern hospitals, such as our new Mott Children’s Hospital have been built for contingencies of terrible new epidemic possibilities such as SARS and Ebola, as well as resurgences of ancient ones like measles – perplexing and only understandable because of persistent human folly. Contagious hospitals revived in Wuhan and Manhattan this winter, although they seem to be more contagious dormitories rather than hospitals as we now think of them.
Three.

A May birthday. One birthday to recall this month is that of Dorothy Mary Crowfoot Hodgkin, born on 12 May 1910 in Cairo, Egypt. I first became interested in Hodgkin when I saw a painting of her at the National Portrait Museum in London, last winter during a visit for the wedding of the daughter of my good friends from our training years in London, Robert and Anita Morgan. The painting was prominently displayed and instantly attractive, but a mistake in the label next to it caught my attention.
Dorothy was the oldest of three daughters of John Winter Crowfoot, a civil servant in the Ministry of Education, and his wife Grace Mary Hood. Living and working in Egypt for many years, the family returned to their native England each summer in the hot months and during one of those summers WWI began. In that August of 1914 the parents left their girls with paternal grandparents near Worthing to return to Egypt, where father could continue work.
After the war, the reunited Crowfoots relocated to Sudan where Mr. Crowfoot was put in charge of national education and archeology, until 1926. The girls attended local schools in Sudan and Dorothy became fascinated by archeology and the mosaic tiles in Byzantine-era churches. She also developed an interest in chemistry and her mother, a botanist, gave her a book on x-ray crystallography for her 16th birthday. Dorothy combined her interests by drawing pictures of mosaic patterns and doing chemical analyses of the tile cubes, called tessera. At age 18 she returned to England to study chemistry at Somerville College, Oxford, and received first-class honors in 1932, proceeding then to Newnham College, Cambridge for Ph.D. studies.
Dorothy worked with John Desmond Bernal on applications of x-ray crystallography to protein analytics and their work on the structure of pepsin turned out to be the first biological crystallographic analysis. Dorothy obtained her Ph.D. in 1937 for work on sterol structure and she held a post as Oxford’s first fellow and tutor in chemistry until 1977. In 1964 Hodgkin won the Nobel Prize in Chemistry. [Below: Hodgkin’s model of penicillin. Science Museum London, Science and Society Picture Library.]
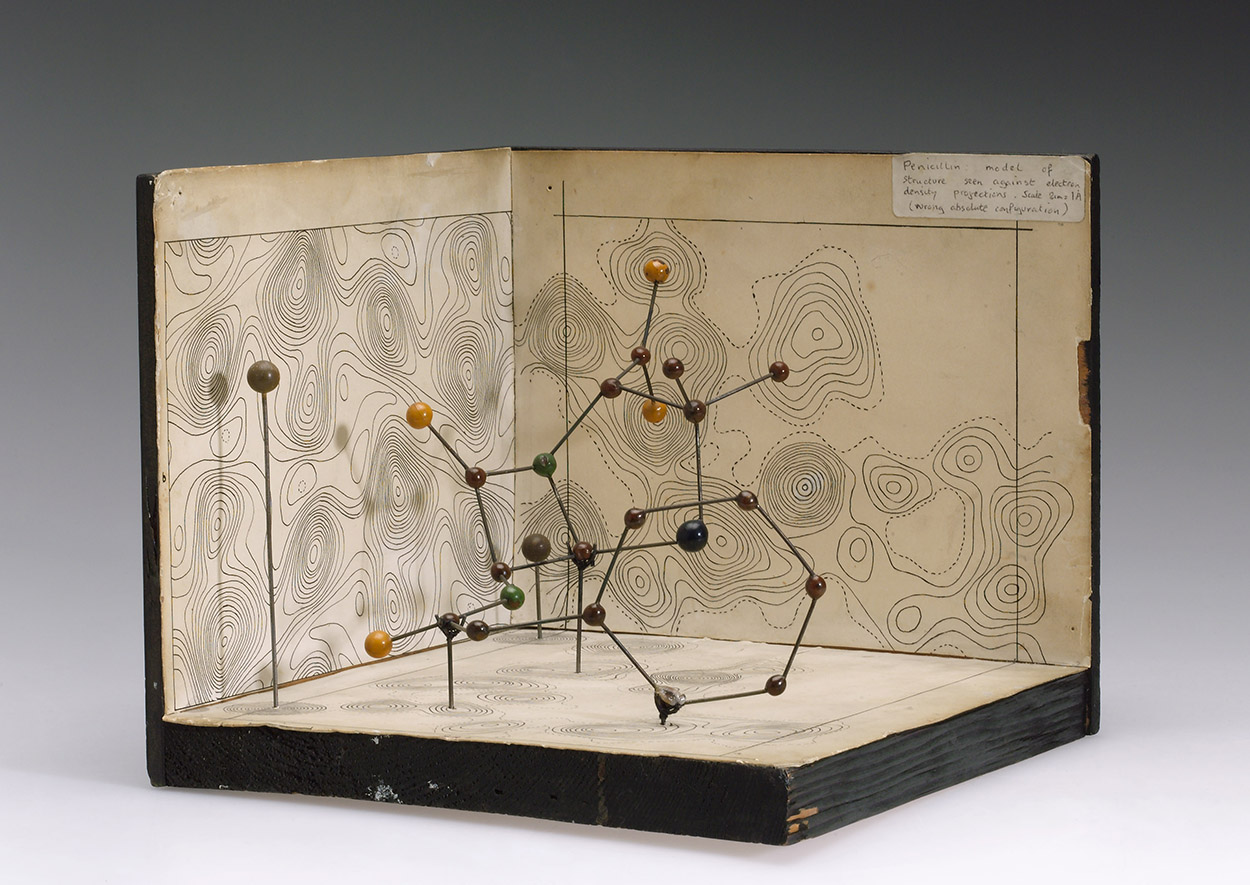
Molecular model of Penicillin by Dorothy Hodgkin, c.1945.
One of her students, a young woman named Margaret Roberts at Oxford from 1943 through 1947, wrote a dissertation on the x-ray diffraction of the antibiotic gramicidin that led to a good job in industrial chemistry but Roberts turned to politics around 1950, married Dennis Thatcher in 1951, and qualified as a barrister in 1953. In 1959, then Margaret Thatcher, she was elected member of Parliament, rising to Prime Minister in 1979. In her office at 10 Downing Street Thatcher displayed a portrait of her former teacher. Hodgkin, however, was a life-long supporter of the Labour Party. [Below: Hodgkin legend with corrected name of artist. National Portrait Gallery London, December, 2019.]
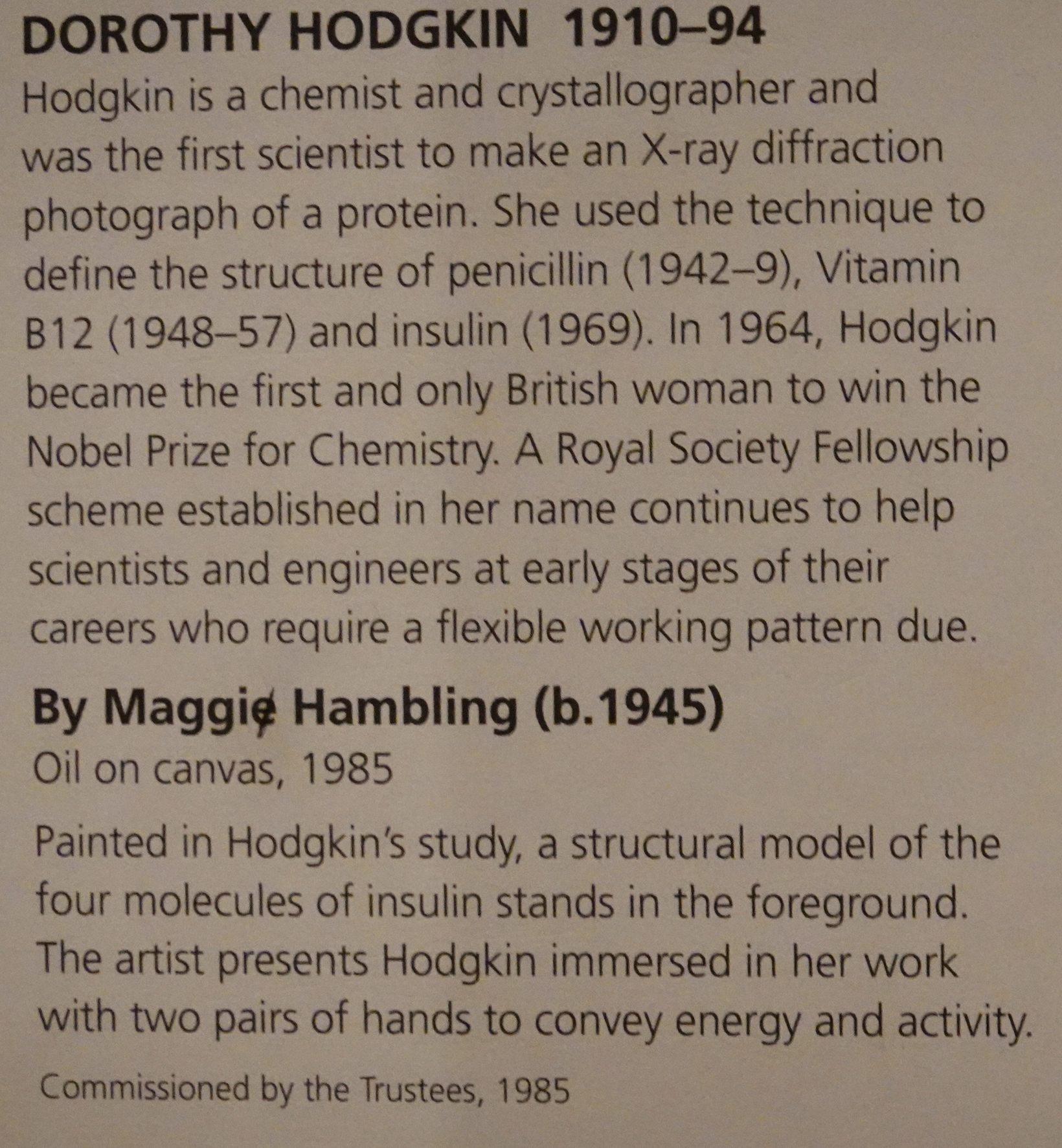
The mistake that caught my eye at the National Portrait Gallery was in the adjacent description of painting and artist, Maggi Hambling, where her first name was written “Maggie,” but someone (I’d imagined it might have been the offended artist herself) crossed out the final “e” with what seemed to be a pencil. No matter, the museum is now closed down for a lengthy renovation and time will likely heal this minor error.
Four.
Among the many innovative changes Ganesh Palapattu has brought to the Department of Urology is the broadening of the weekly grand rounds conferences to periodic wider learning experiences that extend beyond world of urology, that he calls “Teach us something.” A session of this nature in late February featured Professor James Kibbie, Chair of the University of Michigan Organ Department who taught us something in the School of Public Health (SPH) where one of the 16 pipe organs of the University of Michigan temporarily resides. In late February Professor Kibbie spoke on “Bach and the Organ,” and treated our faculty and residents to three beautiful pieces (played on the James Walgreen Létourneau Organ on loan to the SPH) from the 270 surviving organ compositions of Bach. [Above: Professor Kibbie at urology grand rounds.]
Kibbie has been collaborating with computational faculty to understand the science behind Bach’s music and a recent grant from Barbara Sloat allowed him to record all of the Bach organ works, all 270 pieces, performing them on instruments of Bach’s era located mainly in Germany. These works are available to the public through the University of Michigan. [From Prof. Kibbie: “If you want to add the URL for the university’s website with the free downloads of my Bach recordings, it’s http://www.blockmrecords.org/bach.”%5D

[Above: Kibbie, Vesna Ivanĉić, Sam Kaffenberger.]
The pipe organ, complex and large, manipulates forced air through many ingenious pipes. Mistakes are inevitable in all spontaneous performances and Professor Kibbie explained how organ recitals are particularly susceptible, having three keyboards, multiple stops, layers of foot pedals, hundreds or more pipes, and up to 100,000 parts. Paired with the human factor, pipe organs offer countless opportunities for performance variations and transcription errors. Of course, Professor Kibbie’s ear can register musical mistakes that fly by most of us with untrained attention.
Everyone makes mistakes from the moment they arise in the morning, whether squeezing out too much or too little toothpaste, rolling through a stop sign on the way to work, or parking too close to an adjacent car – the possibilities are myriad although most are inconsequential. Error is something we understand in clinical work. Medical mistakes may be transcribing errors when writing (now, typing) patient stories, missing veins on blood draws, or making erroneous clinical decisions. To err is human, to err consequentially is unfortunate.
Algorithms promise perfection, if we are naïve enough to forget that they are written by humans. Whereas a piano played spontaneously offers novel idiosyncratic momentary interpretations, innovations, or mistakes that combine to make each performance unique – and mistakes are nearly inevitable – a programmed piano (player piano) is free of performance interpretation and variation. The standardization (assumed to be error-free, but any algorithm is only as good as its author) brings freedom from the anxiety and art of human performance.
Five. 
A scarlet tanager showed up in our old neighborhood last May around this time. My neighbor, Mike Hommel, called to alert me one Friday afternoon when I was indoors on the computer working on the Urology Department history. Mike is a great naturalist who can spot morels on the ground and birds in the trees better than anyone I know and that day, specifically 10 May 2019, he spotted this little fellow, tired and resting after a long flight from somewhere in the south. The splash of color is amazing and has served its evolutionary purposes well. This little guy was not too concerned by our attention as it shifted trees periodically and hopped to the ground to feed from time-to-time.
Had William Carlos Williams spotted a scarlet tanager on his road to the contagious hospital, the poem would probably have been much different. (Such are the contingencies of life.) Piranga olivacea used to be categorized in the bird family Thraupidae within the Passeriformes family (the perching birds with one backward and three forward toes) but DNA studies have reclassified them to the cardinal family (Cardinalidae). When I was younger the Linnaean binomial classification held little interest for me, but my perspective has changed. I looked for the tanager the next day, but he had moved on. A number of deer, however inspected me carefully. They used to drive us crazy, eating everything we planted, and either we would shoo them away or our dog, Molly, would give chase. By May, 2019, Molly’s arthritis had erased her interest defending the property and at that point the property seemed to belong more to the deer than to Molly or us, which was just as well for we had sold the house to downsize in downtown Ann Arbor.

Other hopeful signs of spring popped up last month, oblivious of the prevailing RNA threat to humans. [Above and below: early April 2020, Ann Arbor Water Hill area.]

[Above: pond in West Park. Below: new normal – outdoor picnic tables at Zingerman’s replaced by spaced waiting areas for take-out orders.]

Postscript.
Disruption. Is clinical medicine a performance art, as aspired to by professionals since Hippocratic times, or is it becoming an algorithmic practice? Professor Kibbie provoked this question. The doctor-patient relationship has been disrupted by the “encounter” framed by the electronic health record (EHR) format, that is the ubiquitous EHR-directed patient “encounters” have replaced the narratives my generation was taught to elicit. We used to initiate evaluation of patients using the so-called SOAP notes (subjective, objective, assessment, and plan) that align with the medical gaze – Sherlockian/Oslerian scrutiny by a trained observer.
A “chief complaint” was a story that could be boiled down to a phrase, but narrative demanded more and gave the chief complaint context. Shoulder pain could be a malignant metastasis or a rotator cuff injury and it was important to know if the injury was life-style related, due to occupation, or traumatic; the story behind the pain, its comorbidities and social determinants, are no less relevant than the pain itself. Abstraction of a patient’s story to a drop-down phrase or an ICD-10 numeric diagnostic code is a poor substitute for conversation, medical gaze, and narrative. We should resist this terrible trend as best we can and create EHRs that support narrative inquiry and medical gaze rather than commoditize encounters.
One hundred years ago, Hugh Cabot got off the train from Boston at the old Ann Arbor station (shown at the top) and initiated the first century of Michigan Urology, not knowing that he would have little more than a decade to do it. Medical care had its disrupters back then, new technology, burgeoning subspecialties, and novel models of practice. Some tension existed between the old and the new approach to disease. Classical Oslerian ideas are routed in the bedside medical gaze and dialogue with the patient to understand and explain the problem. The new scientific approach sought to understand disease based on facts derived in research laboratories, other sources of verifiable data, or from the patient as a virtual laboratory. Clever clinicians recognize it is not a matter of one or the other, patients deserve both approaches. Brutal realities of a post-covid19 world will favor the curt, transactional, commodity aspects of health care. Role models in fiction and fact such as Sherlock Holmes and William Osler, and new analyses such as The Good Doctor – Why Medical Uncertainty Matters, a book out soon by Kenneth Brigham and Michael Johns, help navigate this new era of disruption.
[Below: sign of spring, late April, near Barton Pond.]

Thanks for reading Matula Thoughts of May, 2020.
David A. Bloom, University of Michigan Department of Urology
