
Matula Thoughts
February 5, 2021
2311 words
One.
 One.
One.
February made me shiver… Of all the songs and phrases that accompany most months, this timely phrase from Don McLean’s 1971 song American Pie echoes especially strongly in the minds of many of us who lived through that era of American political unrest and the Vietnam War. I was a surgery intern in Los Angeles back then when the song was making its rounds and even though I didn’t fully understand all of its imagery, the lyrics and music struck a responsive chord. In fact, I wasn’t clear if it was a musical poem rich in metaphor or a pleasing musical jabberwocky of nonsense.
At eight minutes and 36 seconds, it was a long song but the words were authentic for my generation. McLean was only 26 years old at the time, but nostalgia dominated the first paragraph, celebrating the music of “A long, long time ago” before the cold snap mentioned in the second paragraph, “But February made me shiver,” referring to the plane crash that killed legendary singer Buddy Holly on February 3, 1959. McLean’s phrases and tune come back to me every year at this time. [Above: Don McLean singer. Below: Donald Maclean surgeon, UM Bentley Library.]
Two.

Another Donald Maclean (1839-1897), a surgeon unrelated directly to the singer, played an important part in the story of Michigan Medicine. Born in Canada to Scottish parents, this Maclean attended Kingston College in Ontario. He studied medicine in Edinburgh, Scotland and fell under the spell of the great surgeon and teacher, James Syme, who had earlier taught Joseph Lister (Syme’s daughter Agnes married young trainee Lister). Maclean returned to Kingston as professor of surgery but came to Ann Arbor in 1872 as fifth sequential replacement for the founder of UM surgery, Moses Gunn. Unlike the previous short-term intermediaries, Maclean had staying power in Ann Arbor, lasting until 1889 and teaching a generation of UM medical students in the Pavilion Hospital, including William Mayo (UMMS 1883). Just as his predecessors in the Ann Arbor Surgery Chair, Maclean managed his private practice in Detroit and commuted by train to Ann Ann Arbor for classes and teaching demonstrations. Accordingly, Maclean was one of the strong voices who wanted to move the clinical teaching programs and professional practices of the UM medical faculty to Detroit with its larger population and relative abundance of hospitals.
Dean Vaughan, university president James Angell, and the UM regents had a contrary vision of retaining the medical school, clinical practice, and hospital in Ann Arbor, so when the issue came to a head, Maclean and the other “exiteers” were no longer welcome on the faculty. It was at that point that UM established a “full-time” faculty position and university clinical practice for its next chair of the Surgery Department, Charles de Nancrede, who would serve from 1889 to 1917. The university also recognized the need for a more modern hospital facility, and that opened on Catherine Street in 1891, although it quickly proved inadequate for the needs of the times. After de Nancrede retired in 1917 Cyrenus Darling provided a weak interim period of leadership until 1919 when the next chair would be the celebrity urologist Hugh Cabot.
Three.
A paradigm shift occurred between the eras of surgeons Donald Maclean and Hugh Cabot in Ann Arbor. It actually wasn’t such a terribly long long time ago in the grand scheme of things although, to contemporary medical students and trainees, Maclean’s era certainly must seem to be the distant past. Actually, that was the time of my great-great-grandparents.
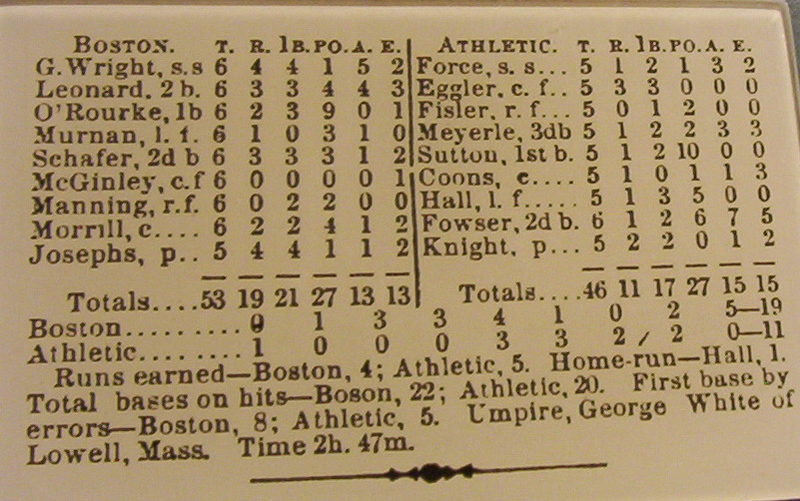
Horace Davenport, UM’s great physiologist and historian of the Medical School, uncovered representative surgical cases of Maclean at UH in 1881-1882, that were published in Physician Surgeon by Maclean. The range of procedures is remarkable considering that Maclean was the sole surgeon and the surgical facilities in the Medical School and Pavilion Hospital were rudimentary. Maclean’s attention to reporting of results, although also rudimentary by today’s standards, was laudatory for his times. [D. Maclean, “A tabular statement of the surgical work done in the Department of After Maclean 1881 and 1882,” Physician Surgeon, 5 (1883): 387-396.] [H. Davenport, Not Just Any Medical School, p. 20.]
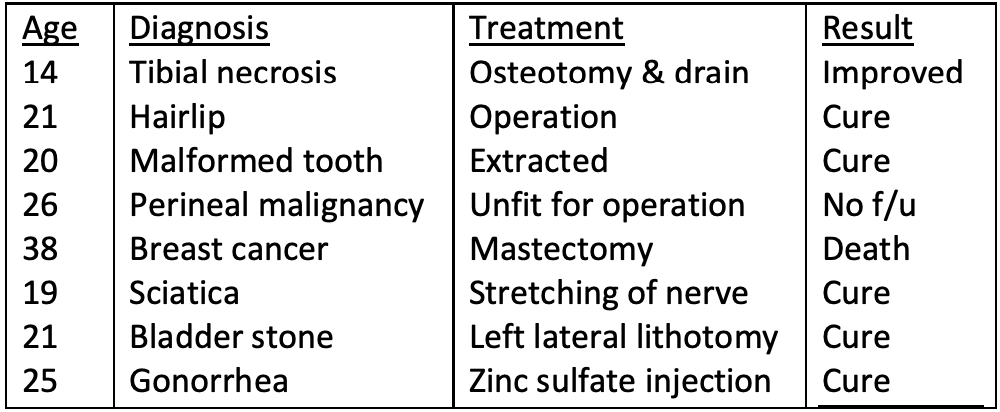
The astonishing paradigm shift that followed Maclean delivered surgical (and medical) specialization to mankind and the first steps of minimally invasive surgery – most widely and effectively evidenced in the urology arena.
Hospitals that were once dormitories for the sick became complex healthcare factories with a multiplicity of diagnostic and therapeutic capabilities. Costs escalated greatly and new parties eagerly began to divide up the monetary pie of health care. Research embedded in medical schools and hospitals generated new knowledge and tools. Medical education expanded from four years of medical school to internships and residency training programs equivalent in length of time or greater than that of medical school. Teams replaced individuals as health care providers. Public health joined with individual health care as responsibilities of modern societies and myriad systems (small practices, community health centers, medical centers, and large healthcare networks) self-assembled to create the modern and postmodern meta-systems of health care in the U.S., Canada, and other nations of the world.
Four.
Hospitalization today is a commonplace phenomenon. In Maclean’s time hospitalization was unlikely for an individual in their lifetime. In modern times, however, most people in industrialized nations are likely to undergo hospitalization at some point in their lives for childbirth, surgery, trauma, cardiopulmonary conditions, infectious diseases, or a wide variety of other conditions.
A friend endured a difficult (non-Covid) hospitalization this winter, emerging successfully but not without much suffering, a number of failed communications, fumbled hand-offs, and errors. All that that provoked another friend to make the common observation that “the system is broken, and broken beyond repair.” Happily, our first friend (the patient) made it home, even as the concomitant covid syndemic exploded, driving UM and St. Joe’s daily inpatient Covid patients above 100 each for the first time since spring.
I feel responsible for our organizational imperfections my friend endured, even though I’m no longer in a position of organizational responsibility. When our Faculty Group Practice (FGP) evolved in the early 2000s I believed that our new UM clinical leadership structure could provide the best hope for aligning the complexities of modern health care to the triple academic mission while taking into account the harsh economic marketplace and changing public policies. Now, as our FGP has become the UM Medical Group (UMMG) under the banner of Michigan Medicine, I still believe this is true, although we have a long way to go, as evidenced by my hospitalized friend.
After I apologized for our systemic imperfections of fumbled “hand-offs” and glitches in processes of care to my friend and his family, I reflected on the common phrase that “the system is broken.” The sad familiar phrase is nonspecific and unhelpful – what actual system was being referenced as broken? It’s almost like observing that the planetary environment “system” is broken, which may well be true, but doesn’t offer much help in solving the universally recognized problem. More accurately, many systems actually work very well, but mainly in serving their own particular needs rather than needs of individual patients and the public at large.
The vast array of enterprises and systems in national health care are variably interconnected, but not united operationally to produce the purposeful and elastic system that we crave. The idea of a single centralized (governmental) system to fulfill the myriad needs of a nation’s health care is not easily imaginable when it comes down to specific functions, in fact that experiment has been tried and failed in 20th century China and Soviet Russia. It doesn’t seem reasonable to think we could build (even with Artificial Intelligence) a systemic set of rules, laws, and organizations to deploy the myriad aspects of personal and public health care, accounting for the needs of workforce education, research, innovation, public policy, crisis preparedness, safety nets, private sector, and professional organizations.
We presently witness the astonishing multinational development of multiple effective vaccines in response to the global pandemic, decelerate in the implementation phase with clumsy national and local policies, supply chain issues, political rhetoric, false narratives, vaccine deniers, and worldwide healthcare disparities resulting from poverty and racism. A tiny virus has thrown every national and health care system into states of confusion and exacerbated the known inadequacies and disparities.
Five.
Making health care work. The charge that “our system is broken” is aimed most acutely at the fundamental parts of health care – the delivery of individual ambulatory and inpatient care, while supporting the public health of a population. It is a certainty that any given integrated organization, such as Michigan Medicine, can go a long way toward making health care work better and more fairly for their individual patients, workforces, and regional stakeholders.
The operation of a large regional health care system such as Michigan Medicine is not amenable to any algorithms known to mankind. Expectation that artificial intelligence might provide efficient and humane central management will likely be disappointed, just as other exclusive central systems failed to provide societies the full range of health care in its particular clinical, public, educational, investigative, and innovative dimensions. It’s difficult to identify any society that has pulled off this pent-fecta, although it’s not for lack of trying. For now, the best hope is management by teams that distill content expertise of specialties and stakeholders, to aligning them to the needs of the individual patient, the public health, and the larger aspirations of society.
It was big news at UM in Ann Arbor in mid-month when David Miller was named as President of Michigan Medicine, taking over from David Spahlinger, who had done great service in the role of President of UMHS and Executive Vice Dean for Clinical Affairs, a position he held in its various names through two decades of astonishing change and growth. [In modern health care camouflage: above David Spahlinger and below David Miller and Justin Dimick.]
Postscripts.
Another Donald Maclean (1913-1983) evokes the spirit of the late David Cornwall. This Maclean was a member of a Cambridge spy ring that passed British and American secrets to the Soviet Union in WWII and during the cold war. The Gaelic surname in its various spellings means alternatively ‘son of Gillean’ referring to Gillean of the Battle Axe of Ireland around 1200 or ‘servant of St. John.’ The Scottish Clan MacLean has been powerful throughout the history of Scotland and all the MacLeans, Macleans, McLeans, McCleans, McLaines, and McClains may well derive from a single mitochondrial mother “Eve.” [Below: Donald Maclean the spy, Wikipedia.]

Maclean made headlines in 1951 when he exfiltrated to the Soviet Union, along with fellow conspirator Guy Burgess, and they would be followed in 1963 by Kim Philby. Maclean’s family accompanied him to Moscow but after an affair with Philby, Mrs. Maclean returned to the West 1979, dying in NYC in 2010. The three Maclean children each married Russians, but all subsequently also returned to the West, leaving their father behind, working as a foreign policy analyst at Moscow’s Institute of World Economy and International Affairs. He died, reportedly of cancer at age 69, and was cremated and honored in Moscow in 1983.
A Fourth Man, fellow spy Sir Anthony Blount and art historian and Surveyor of the Queen’s Paintings, stuck it out in England and was unmasked in 1979, but lost only his knighthood. The Cambridge Four later turned out to have been the Cambridge Five, after John Cairncross (code-named Liszt) was confirmed by KGB defector Oleg Gordievsky in a 1991 interview as the Fifth Man. Cairncross, a literary scholar from Cambridge had previously been known as an atomic secrets spy, confessing partially in 1951 and losing his civil service job. He moved to the U.S. as a lecturer at Northwestern and Case Western Reserve, where he confessed more completely in 1964 to British investigators who had opened his case after Philby’s defection. Cairncross moved to Rome in 1967 to work for the U.N. and then in 1970 to Provence, France. He died in England in 1995.
These convoluted truths may seem stranger than fiction, but made for great stories from the late great spy novelist John le Carré, the pen name of David Cornwall (19 October 1931 – 12 December 2020) in the enduring tales of George Smiley and other memorable protagonists.
February each year manages to get the work of a month accomplished in fewer days than the other longer months. This, of course, is a hyperbolic thought, as if a month is a purposeful agency instead of an arbitrary block of time. Yet, this playful conjecture is an inverse run of Parkinson’s Law by which work expands to fill the time or other resources available for its completion.
Parkinson, a British naval historian and academic in Malaya, in his later career, wrote a short piece in the Economist in 1955 that he expanded into a book in 1957. He thus fulfilled his own law – expanding words rather than more vaguely defined work – to explain the same idea of Parkinson’s Law, laid out in the brief Economist article, later in his book.
Like most rules of organizational theory, Parkinson’s Law needs to be taken with the proverbial grain of salt, although Parkinson took it pretty far, mathematically modeling it out based on an analysis of the British Admiralty staff from 1914-1954. He considered how the administrative staff grew inexorably, unrelated to number of commissioned ships, wars, or other obvious factors: more personnel, but no additional work. His formula predicted that management staffing increased annually on an average of 5.75% (with a modeling range of 5.17 to 6.5%) regardless that the amount of work was static, without annual increase, but factoring in ages of appointment and retirement, and man-hours required for communication among personnel.
Parkinson’s self-styled rule, was greatly (but not entirely) satirical, much like Willie Sutton’s rule for success (go where the money is) or Robert Sutton’s organizational No Asshole Rule (don’t retain “jerks” in the organization) for successful teams.
Thanks for reading Matula Thoughts, this February 2021.
David A. Bloom, University of Michigan, Ann Arbor




















{kind=link}