
DAB What’s New January 6, 2017
Free, efficient, and equal government
3752 words

One.
Let’s not leave 2016 without a few comments about December. At Grand Rounds Andrew Peterson, visiting professor from Duke, and Daniela Wittmann gave excellent presentations on urologic cancer survivorship. Andrew explained his remarkable survivorship/reconstructive fellowship in Durham and Daniela gave a 10-year review of our uniquely successful Brandon survivorship program.

Medical students raise money for our Galens Society annual “Tag Days” in early December. Founded in 1914, Galens supports Mott Children’s Hospital and other organizations that benefit children in Washtenaw County. [Above: Paul Cederna of Plastic Surgery with MS1s Alex Tipaldi and Michael Klueh at the Taubman 2 Urology ACU.]

Our holiday party at Fox Hills entertained over 350 people with the expected surprise of Santa who had gifts for all the children (above). Pat Soter, her husband Jim, as well as Sandy and Bob Heskett, did the heavy lifting for this event and we thank them. Pat’s retirement leaves a major challenge filling her shoes. A faculty evening meeting (below) discussed residents progress, urology divisions, strategic planning, and John Stoffel’s stint as Acting Chair.

Now that we are 6 days into 2017, Happy New Year from Michigan Medicine’s Department of Urology.
Two.
Liberty, once attained, is taken for granted. We grieve its loss, fight for it, but are not good at maintaining it. On this day in 1941 Franklin D. Roosevelt delivered his Four Freedoms State of the Union address. Pearl Harbor would happen 11 months later. FDR came to the presidency in turbulent times and became enormously popular, serving nearly 4 terms. Some people disparaged his social policies, yet few disputed his belief in essential freedoms: freedom of speech and expression, freedom of worship, freedom from want, and freedom from fear.

[Washington @ Delaware. Sully 1819. Boston Fine Arts Museum]
The State of the Union address is prescribed by Article II Section 3 of the U.S. Constitution. George Washington gave the first to Congress in New York City on January 8, 1790, 9 months into office. The new government had recently come to power after 11 of 13 states accepted the Constitution, but North Carolina waited to ratify, pending a Bill of Rights. Washington’s address, praised North Carolina’s acceptance two months earlier. (Rhode Island became the last of the 13 original colonies to ratify, later that year on May 29.) That first State of the Union address at 1089 words (page 1 below) is shorter than any of its successors.
Washington set the tone in the opening sentences.
“Fellow Citizens of the Senate, and House of Representatives. I embrace with great satisfaction the opportunity, which now presents itself, of congratulating you on the present favourable prospects of our public affairs. The recent accession of the important State of North Carolina to the Constitution of the United States (of which official information has been received) —the rising credit and respectability of our Country — the general and increasing good will towards the Government of the Union —and the concord, peace and plenty, with which we are blessed, are circumstances, auspicious, in an eminent degree to our national prosperity.”
The conclusion was optimistic.
“The welfare of our Country is the great object to which our cares and efforts ought to be directed. And I shall derive great satisfaction from a co-operation with you, in the pleasing though arduous task of ensuring to our fellow Citizens the blessings, which they have a right to expect, from a free, efficient and equal Government.”
We anticipate President Trump’s State of the Union will seek reconciliation of political polarities without yielding on core issues that decided the election. Healthcare will be heavily weighted to the legislative agenda of Paul Ryan and operational agenda of HHS head Tom Price (UM alumnus and orthopedic surgeon).
Three.
Year 1 UMMG. The ability to practice and innovate in healthcare drew many of us to medical careers, but these freedoms have become constricted. Specialization, systemic organizational impingements, economics, and regulation drive much of the constriction. Some laws restrict conversations between patient and physician, as if healthcare providers were agents of government rather than citizens with first amendment rights (after all, free speech was first in the Bill of Rights).
Consumer discontent over healthcare delivery dominates the news, but discontent from the perspective of practitioners is equally important; dissatisfaction within healthcare professions affects delivery, efficiency, education, innovation, and pipeline of future practitioners. We can’t solve all the national and regional healthcare problems from Ann Arbor, but we can influence their solution and serve as a best-of-class example.
The structure, governance, and policies of the UM Health System have re-assembled over the past year. Our new Michigan Medicine governance is certainly less monumental than Washington’s new union in 1790 and contains key differences. Whereas the US federal system depends on a three-way balance of power, Michigan Medicine intends an integration of authority. “Silos” that evolved over the past 150 years at UM – namely the Medical School (UMMS) and its faculty, clinical departments, hospital administrative structure, and research enterprise – while related and sharing many of the same people, often worked at cross purposes to defend budgets, becoming archipelagos of cost centers.
One year ago the UMMS and its Health System merged the positions of Dean and EVPMA (Marschall Runge). Three vice dean positions were created: Clinical Vice Dean/President of UM Health System (David Spahlinger), Academic Vice Dean (Carol Bradford), and Scientific Vice Dean (TBD). A new UM Hospital Board with healthcare expertise and regental participation will oversee the entire health system and medical school.
The re-organized health system has 3 main operating units: Hospital Group I (Main & CVC), Hospital Group II (Mott & Women’s), and the UM Medical Group (UMMG, formerly the Faculty Group Practice = FGP) that manages ambulatory practices as well as regional affiliations. In the 2007 FGP, UM ambulatory activities were divided into 90 Ambulatory Care Units (ACUs) intended to function under local control by the healthcare providers to maximize lean principles. The ACUs have grown to 150 and Timothy Johnson was just named UMMG Executive Director. Tim ran the Multidisciplinary Melanoma Program, served as Division Chief of Cutaneous Surgery and Oncology, led the very successful Mohs Ambulatory Care Unit director, served as training director of the ACGME fellowship in Micrographic Surgery and Dermatologic Oncology, and is the Lewis and Lillian Becker Professor of Dermatology.
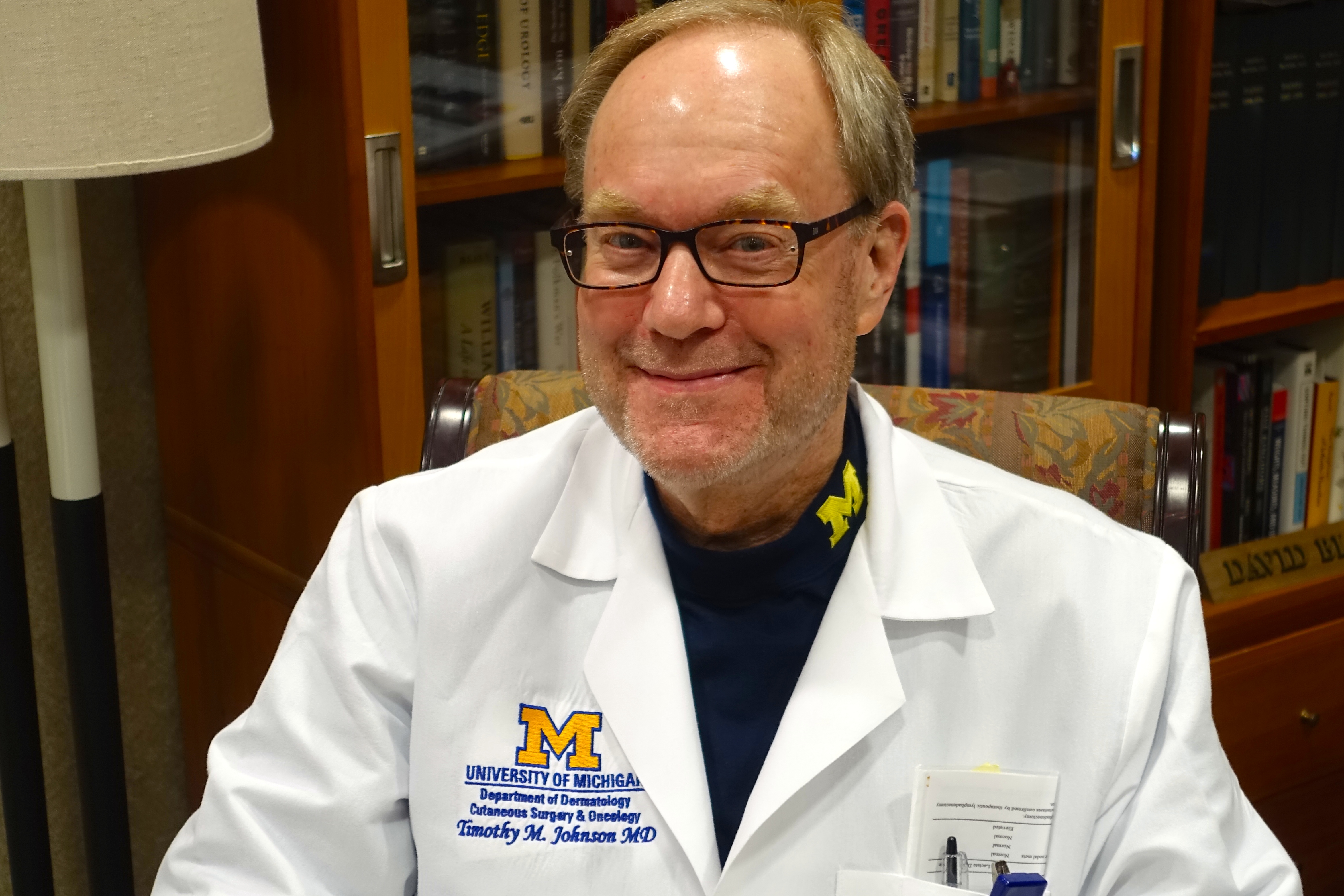
Tim’s skin cancer programs involve over 25 departments, divisions, service lines, and centers, and consistently earn superb ratings of patient satisfaction, employee engagement, and access. His programs generate significant grant funding, publications, and clinical trials.
New governance structure, expanded facilities, and growing affiliations should allow Michigan Medicine to carry out its missions no matter how the greater US healthcare system evolves. The UM has a history of innovative morphology beginning in 1869 when a faculty house became a hospital – the first occasion for a university to own and operate a hospital. While this originally happened for the purpose of teaching, the mission evolved to become a conjoined one of education, research, and state-of-the-art clinical care.
Four.
Inclusion of a hospital within the Medical School, extended medical education from classrooms to bedsides, a first step in building the UM Health System. Clinical and investigational laboratories later brought science into medical education and created new opportunity for investigation and innovation. An ambulatory care building in 1953 and offsite clinics carried UM into outpatient healthcare that is now expanding into homes, workplaces, and other daily living spaces of patients. This fourth dimension of healthcare (1=classroom, 2=bedside/OR, 3=ambulatory clinic, and 4=patient life circumstances) complements health services research, as practiced in our Dow HSR division, opening doors between medical schools and schools of public health, pharmacy, natural resources, nursing, kinesiology, and sociology. Our North Campus Research Center (NCRC), acquired from Pfizer, facilitates integration of all healthcare dimensions. [Below: David Canter Executive Director NCRC & Marschall Runge]

Five.
Polar arguments related to the future of health care are being fought simultaneously in political battlegrounds and marketplaces. One argument is that health care is “too expensive” and we often hear that “we’re giving too much away.” The other argument was summarized in The Lancet cover quotation just before the November election: “Whichever way the election goes, one issue is certain: the next president of the USA will inherit a country in which deep health and health-care inequalities exist along multiple lines, including income, race, and gender.” [Editorial. “America decides.” The Lancet. 2016; 388: 2209]
There is little doubt that healthcare as deployed today is expensive and many factors account for this, significantly the insurance-based paradigm, corporatization of healthcare, and regulatory costs. Fee-for-service (FFS) factors and waste in the system are also blameworthy. Although both can be mitigated, waste will never be eliminated in human processes and FFS always finds a place in any free society. When people complain that too much is being given away, they are likely referring to suspicion that “other people” benefit from services that they, as taxpayers, support. This sense of unfairness is deeply seated.
Just as deeply seated at the other pole of belief is outrage over the unfairness of healthcare disparities. The right to healthcare, many will argue, is essential to life, liberty, and the pursuit of happiness, ideas deeply ingrained in American civic belief. No less important is the fact that it is in the public interest for everyone to have a basic level of health care. It is in your interest that the person next to you, next to your family members, next to your colleagues, and next to your friends – whether on the street, in a store, at a restaurant, or on a plane – doesn’t have TB, measles, Ebola, or some other communicable disease. It is in all of our interests that air and water quality are good. It is in our interest that violently mentally ill people are not disrupting work places or driving on streets. It is in your interest that homeless people have health care. Every civilized country recognizes some national responsibility to provide health care, differing mainly in the mechanisms and extent of coverage.
Reconciliation of these polar beliefs is a political problem, an economic problem, and a public policy problem. No simple solution or model will likely satisfy all these problems and beliefs. The public wants availability, affordability, and quality, but finds it easier to provide any two of these attributes instead of all three.
Six.
Federally Qualified Health Centers (FQHCs) provide one avenue to health care. These community-based organizations target underserved health care needs. Established to provide comprehensive health service to the medically underserved and reduce emergency room care, the FQHC mission has shifted to enhance health care services for underserved, underinsured, and uninsured individuals in urban and rural communities. Care is provided to all patients, including migrant workers and non-US citizens, regardless of ability to pay, based on sliding-fee scales established by FQHC community boards. In return for serving all patients FQHCs receive government cash grants, cost-based reimbursement for Medicaid patients, and malpractice coverage under the Federal Trot Claims Act (FTCA) of 1946. The ACA set aside $11 billion dollars over 5 years to cover FQHC costs. FQHCs serve one in 13 people in this country.
Some of the approximately 2000 FQHCs in the US are small operations, while others like the Hamilton FQHC in Flint are substantial enterprises. Two federal agencies oversee FQHCs. One is the Bureau of Primary Health Care, under the Health Resources and Services Administration (HRSA). The other is the Centers for Medicare and Medicaid Services (CMS), also under the Department of Health and Human Services (HHS). The Health Center Consolidation Act of 1996 (commonly called Section 330) brought together funding mechanisms for community health facilities, such as migrant/seasonal farmworker health centers, healthcare for the homeless, and health centers for residents of public housing. Previously, each of these organizations was provided grants under other mechanisms.
The Bureau of Primary Health Care is a part of the Health Resources and Services Administration (HRSA), of the United States Department of Health and Human Services. HRSA helps fund, staff and support a national network of health clinics for people who otherwise would have little or no access to care.
The Centers for Medicare & Medicaid Services (CMS), previously known as the Health Care Financing Administration (HCFA), is a federal agency within the United States Department of Health and Human Services (HHS) administering the Medicare program and partnering with state governments to administer Medicaid, the State Children’s Health Insurance Program (SCHIP), and health insurance portability standards. In addition to these programs, CMS has other responsibilities, including the administrative simplification standards from the Health Insurance Portability and Accountability Act of 1996 (HIPAA), quality standards in long-term care facilities (more commonly referred to as nursing homes) through its survey and certification process, clinical laboratory quality standards under the Clinical Laboratory Improvement Amendments, and oversight of HealthCare.gov.
Seven.

The Hamilton Community Health Network (HCHN) began in 1982 as the Hamilton Family Health Center under St. Joseph’s Hospital (now Genesys Health System) in response to unmet healthcare needs in Flint, Michigan. Moving to the present site (now the administrative headquarters shown above) in 1988 it began receiving federal funds to provide healthcare for the growing homeless population. Becoming HCHN in 2001 the organization assumed financial and operational responsibility from Hurley Hospital for primary and preventive care at the hospital’s North Pointe facility, and the following year began operations at a combined medical-dental site in partnership with the Genesee County Health Department. Hamilton, now a part of a national network of primary care centers (Section 330E), provides comprehensive healthcare services for underserved urban, rural, and homeless populations in addition to operating a family medicine residency program under HSRA funding since 2014. Hamilton has 6 clinical sites: the Main Clinic, the Burton Clinic, the Dental North Clinic, the Clio Clinic, the Lapeer Clinic, and the North Pointe Clinic. The Main Clinic is a new $5 million facility of 31,000 square feet, funded by federal dollars, local grants, a capital campaign, and debt that has been totally paid off.
The pairing of urology and primary care practices is natural. The Hippocratic Oath 2000 years ago recognized the unique nature of urologic expertise and the need for specialists. Every human being will have urologic issues of one sort or another and there will never be enough urologists to “go around.” Working side-by-side with primary care providers, urologists can teach them, just as they can teach urologists, providing comprehensive health care where and when it is needed.

[Above: Hamilton FQHC in Flint: Board of Directors. Below CMO Mike Giacalone Jr., CEO Clarence Pierce]

The UM Urology Department began clinics at Hamilton in 2015 working with an excellent clinical team including a superb physician’s assistant Ben Busuito (below). Urology clinics are now staffed nearly every week by myself, John Wei, John Stoffel, Anne Pelletier Cameron, Ganesh Palapattu, Meidee Goh, Chad Ellimoottil, and Gary Faerber – who has been coming back periodically from Salt Lake City. Our faculty have never been assigned to Hamilton nor subsidized to travel to clinics; we simply created the arrangement and our urologists saw the need and the opportunity. My clinic at Hamilton is streamlined for patients and providers, so my time in Flint is also a learning experience to improve our UM ACUs.

[Clinic team: Melanie Slackta, Alice Yanity, Ben Busuito, Michelle Durall, Michelle Williams]
Eight.
True facts. Legendary professor Don Coffey at Johns Hopkins often admonished trainees: “You have to understand the difference between facts and true facts,” advice that resonates with me in this new milieu of fake news on social media. Don taught the importance of critical thinking and insistence on truth. The truth matters in science, in politics, and in all human interactions.
American philosopher Harry Frankfort wrote an important book entitled indelicately, but appropriately, On Bullshit (Princeton University Press, 2005) and this demanded a sequel the following year, On Truth (Alfred A. Knopf, 2006). Both books are worth your attention. (friend at Emory gave me a copy of the former book). If you’ve read them once you should read them again. True facts seem to have diminished influence today and false news is on the rise. Expect change in 2017. Worldwide social media communication will drive much of it, but dig critically for truth and its impostors.

[Oct. 31, 1938: Orson Wells telling reporters no one expected the broadcast would cause public panic. Acme News Photos. Wikipedia]
The infamous War of the Worlds radio play in 1938 is a cautionary tale. The HG Wells story was directed and narrated by Orson Wells (no relation), but listeners who tuned in after the introduction misinterpreted the play as an actual alien invasion. Modern social media technology has increased the ease of dissemination of erroneous stories or deliberate manipulative propaganda. A single false story or conspiracy theory can spread around the planet in minutes to reach a sizable part of our 8 billion gullible global citizens. With print media and professional journalism on the decline, the world is dangerously vulnerable to manipulation by a random or purposeful catalyst.
The best defense against tomorrow’s War of the Worlds will be based on two foundering, elements of civilization. One is education – teaching critical thinking skills. That education needs to begin in grade school and sharpened later on the educational ladder in math, physics, physiology, and pharmacology just as well as in English, art history, or architecture. Broad critical thinking needs to continue in professional schools, graduate medical education, and beyond in our jobs and communities. The other element is a multiplicity of robust, trusted, and critical media sources providing timely scrutiny and analysis – and these are the fourth and fifth estates.
Nine.
Medieval social power structure can be conceptualized to three estates of the realm, namely the clergy, the nobility, and the commoners. The American colonies that united under George Washington disrupted that traditional model to create representational democracy and it is no mere coincidence that one of its early builders was a printer, Ben Franklin. Imperfect as it was and is, representational democracy surpasses anything else that has been attempted for civilized governance, but it demands an educated populace and continuous vigilance by the press, known as the fourth estate.
The immediacy of social media led to the concept of a fifth estate, consisting of web-based technologies. Curiously, that was the name of a countercultural underground newspaper, first published in 1965 in Detroit. The first issue included a review of a Bob Dylan concert, a “borrowed” Jules Feiffer cartoon, and announcement of a march in Washington. The periodical remains active and is believed to be the longest-running anarchist publication in English. The Fifth Estate archives are held here at the University of Michigan in the Labadie Collection at the Harlan Hatcher Library. [Below: First page first edition Nov 19-Dec 2, 1965. Courtesy UM Labadie Collection & Julie Herrada]
————————————————–
What’s New/Matula Thoughts, this particular small-scale electronic posting, was intended as monthly essay for colleagues and friends. It has worked its way around the global village although we can’t track the What’s New email version that gets forwarded beyond its initial recipients, we can track the MatulaThoughts website version through WordPress analytics.
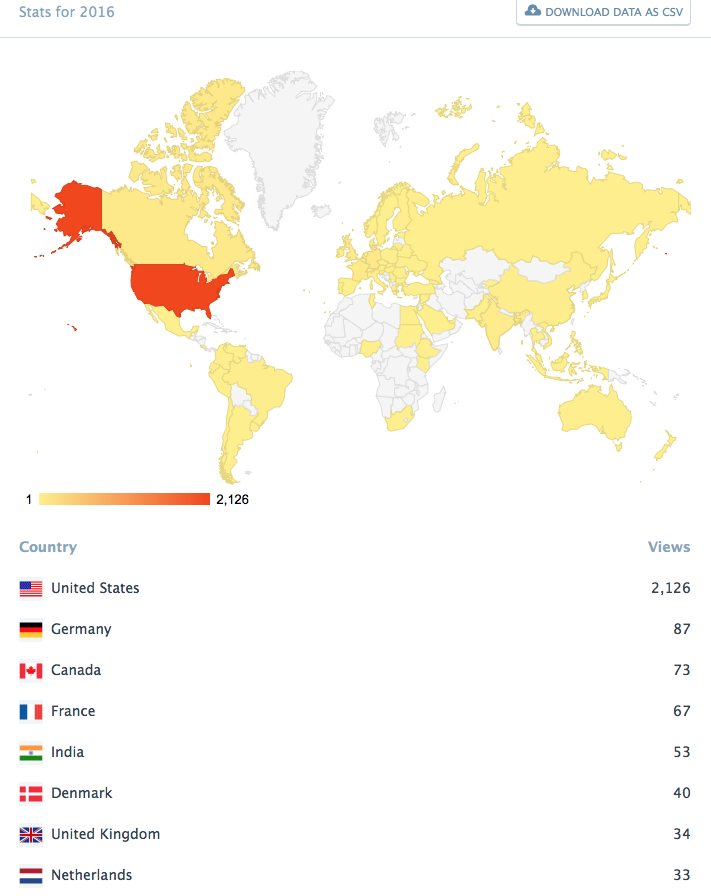
[Above: MatulaThoughts analytics in mid-December]
Most web postings of this sort feature short blurbs linked to aggregated articles that may, or may not, contain verifiable reporting or critical analysis. MatulaThoughts differs in that its 10 items contain some streams of continuity, random observations, and specific references usually to scientific literature. Striving to keep this under 4000 words, we view this as a monthly essay for Michigan Urology family and friends, recognizing that while many find time for only a cursory scan, others pick out one or more items to read more carefully. Some readers around the globe, however, read this better than I write it, and communicate back related observations, different opinions, or find mistakes I’ve made. My thanks, especially, to those critical analysts.
Ten.
The Fifth Estate, just as the fourth, was heralded as a boon to free speech, human liberty, and democracy. Outrageous claims or gross propaganda, however, bring a perverse twist to social media, abetted by public tolerance and even an appetite for fake news. The boundary between fake news (mainly enjoyed as entertainment) and true factual news is indistinct and the difference doesn’t seem to matter to many people. This imperils democracy for it cannot be doubted that truth matters in a free and civilized society. Social media can provoke a presumably rational person to enter a church and open fire on parishioners, to take weapons to “investigate” restaurants in distant cities, to target-shoot highway drivers, or “execute” policemen in their cars. The truth matters to all of us. Its distortion undermines civilization.
Truth matters in science and is absolute in the health professions. Deception in the reporting of a blood test, cut-and-pasted notes, conversations with colleagues or patients, or manipulated scientific results may sneak by in the workplace or in the literature for periods of time, but eventually get discovered and demand public scorn and long-standing distrust. One rascal, even among thousands of “honest brokers” diminishes the public trust. Trust matters in engineering, construction, food safety, nuclear power plants, the transportation industry, water standards, air quality, and so on. It matters too in journalism, law, politics, and life in a cosmopolitan world. Purposeful exploitation of truth, whether self-serving lie, propaganda, or mischief should be called out. A related deception is that of careless or deliberate plagiarism, when another person’s distinct intellectual property such as sentences, images, etc. are claimed as one’s own.
How then can we distinguish these threats to free speech from fiction? To me, fiction is the art of creating a story that entertains and may give insight to our lives. The proper purposes of fiction (that is, the purposes that civilized and educated people should accept) are distinct from propaganda, deception, and plagiarism.
Freedom of speech carries with it the responsibility to be critical and intolerant of gross distortions. Preservation of the freedoms we claim as humans (namely, life, liberty, and the pursuit of happiness) demands an attention that in this country we elevated to a cabinet-level status under Dwight Eisenhower in 1953. This was the Department of Health, Education, and Welfare (HEW) with the motto, “Hope is the anchor of life.” In 1979 the Department of Education was split out and HEW became the Department of Health and Human Services (HHS). These organizations have spent much taxpayer money and have done great good, but are complex and imperfect. These have been, I believe, the only cabinet-level departments created by presidential reorganization. The ability of the president to create or reorganize bureaucracies, as long as neither house of Congress passed a legislative veto, was removed after 1962. Fifteen executive cabinet-level departments currently exist.

[Above HEW seal; below HHS seal]

Although seemingly arcane, these matters demand our attention for a free, efficient, and equal government.
David A. Bloom
University of Michigan, Department of Urology, Ann Arbor









