WN/MT July 3, 2020
Origin stories
2518 words

One.
Hunkering down this spring, we explored Ann Arbor’s Water Hill neighborhood during social-distanced walks and saw flags that anticipated the Fourth of July. Tomorrow’s holiday brings to mind Danielle Allen’s book, Our Declaration. The American national origin story centers around a representative democracy formed disruptively when 13 colony-states spun off from a parliamentary monarchy. Even at the start, the story was complicated by the colonial expropriation of lands from their indigenous inhabitants and enslavement of abducted Africans to build the economy. These matters remain unreconciled, and so some Americans today will display the flag upside down, take a knee, or illuminate irreconciliation in other ways.
As the number of states increased in America, state sovereignty contested federal authority over a variety of issues amidst economic crises, wars, environmental catastrophes, epidemics, and paradigm shifts in technology. Life got more complex with technology, subspecialization, regional interdependency, and the sheer scale of rising population. Many matters transcended state boundaries and demanded federal solutions. Consider, for example, a public debate in 1820 on the role of federal government in matters of personal health, public health, medical licensure, specialty certification, and health care economics versus a similar debate today. The debaters in 1820 would have scratched their heads wondering what possible business the government could claim in such issues, except possibly a limited responsibility for public health.
The basic Jeffersonian aspirations within the Declaration, however, seem to hold true and anchor most of the attempted solutions to the nation’s big and little problems. Those personal aspirations – life, liberty, and the pursuit of happiness – bear repetition, especially now in July, 2020. It now takes great rhetorical acrobatics to discount the role of equitable public and personal health care in life, liberty, and the pursuit of happiness in today’s complex world. A debate in 2020 over the roles of federal government in matters of personal health, public health, medical licensure, specialty certification, and health care economics would be quite different than that imagined debate of 1820.
One big effect of this pandemic may be that the public may find a way to build a new vision of government “by the people and for the people” that will fine-tune the aspiration of “life, liberty, and the pursuit of happiness” to the complexities of 21st century civilization. Governmental responsibility for “life, liberty, and the pursuit of happiness” entails securities of personal freedoms, food, and employment, as well as public safety and public health. Any line placed between public health and personal health, or between public safety and personal safety is an arbitrary choice. These basic securities should be expected of any state or society, worthy of the term civilization.
Two. 
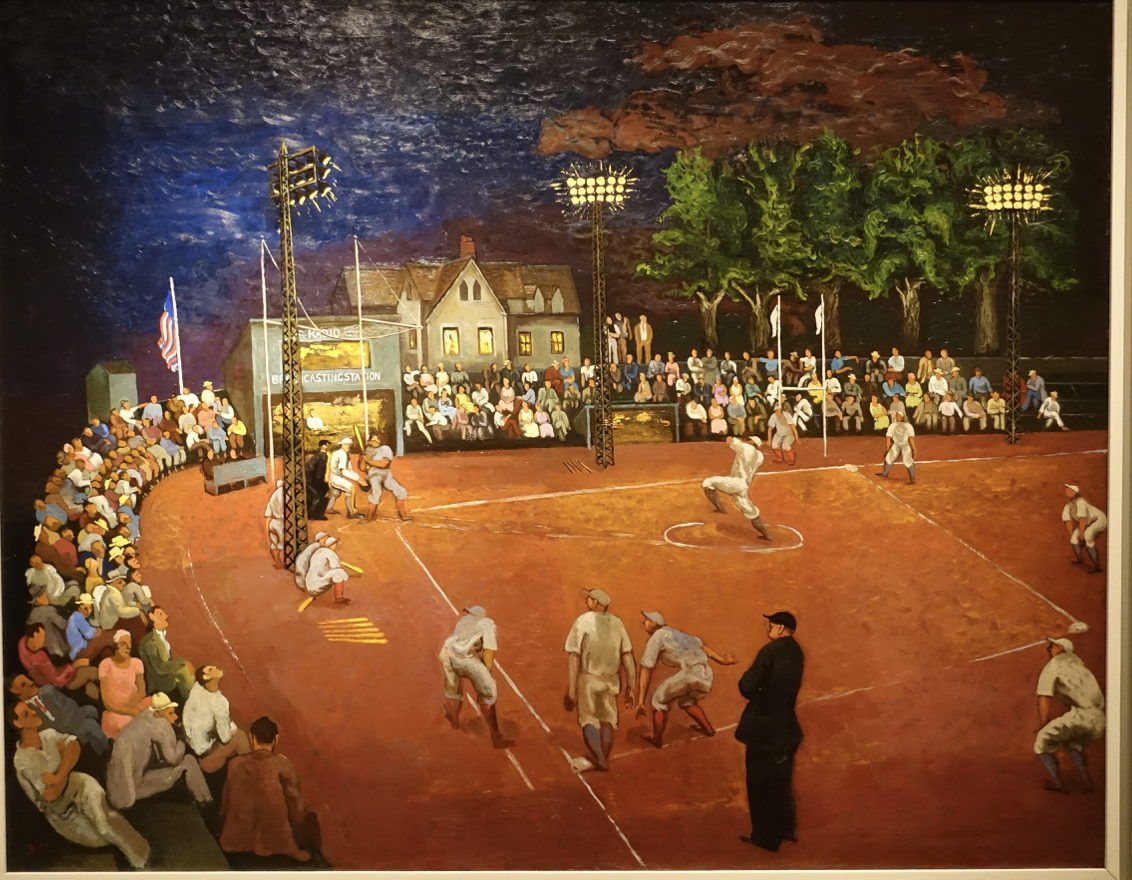
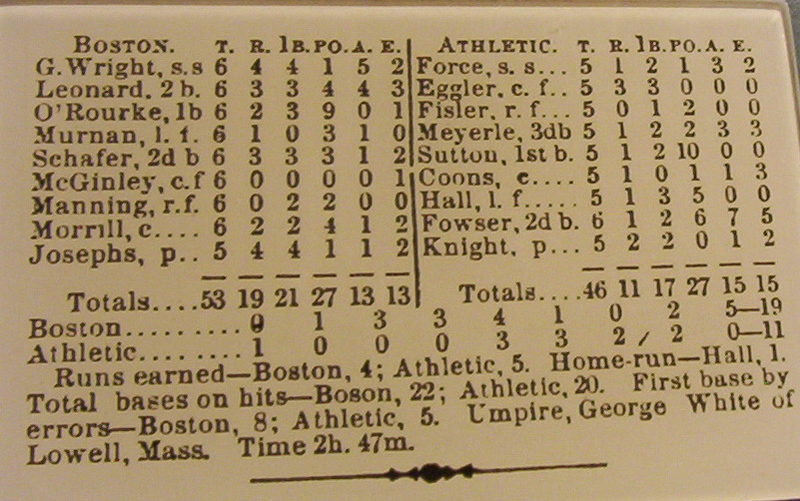
Baseball comes to mind now, but this season is off to a slow start, if it happens at all. So meanwhile, a bit of time travel to the past is in order: a little more than ninety years ago (May, 1930) Ty Cobb threw out the first pitch at a new baseball park in Hamtramck, Michigan. [Picture below: 1928 International Newsreel photograph of Lou Gehrig on left, Tris Speaker, Ty Cobb, & Babe Ruth taken in April 1928.]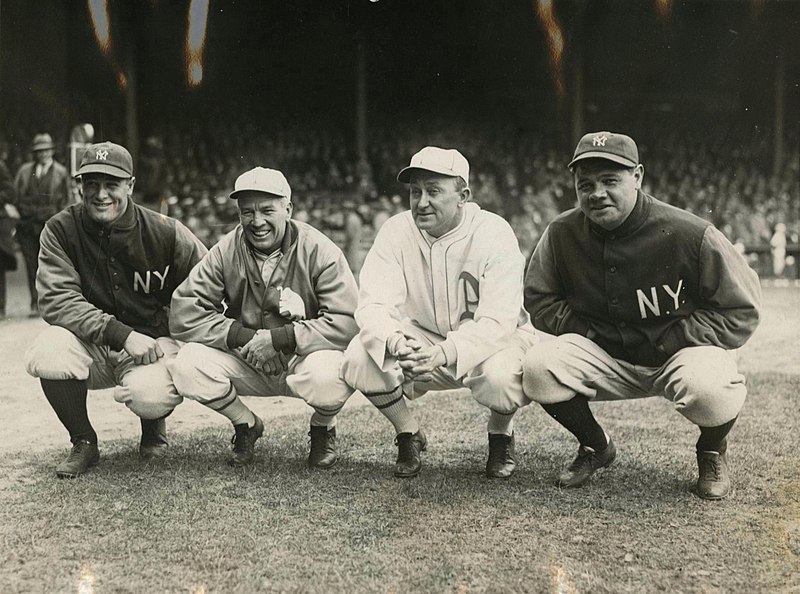
Cobb was a national celebrity who had retired from the Detroit Tigers in 1928 after 22 seasons and came back for opening day at Hamtramck, although he never actually played a game there. The new stadium, replacing Mack Park, would serve as one of the historic Negro League venues through 1951.
Mack Park had been home to the Detroit Stars, but after the grandstand burned down in 1929 the venue was relocated to the Hamtramck site, opening in May 1930. The Detroit Wolves took over for the Stars, in a new East-West league in 1932, but folded in the unfavorable economic times. The Detroit Stars was resurrected in 1933, but lasted only one more season at Hamtramck, that then lay empty. The Stars had a third life in 1937, but that too lasted only one more season. Detroit city acquired Hamtramck Stadium in 1940 and renovated it through Roosevelt’s Works Progress Administration as part of a larger Veterans Park project. Hamtramck Stadium has since hosted high school and Little League games, but after 2012 it fell into disrepair and neglect. Of the 12 remaining Negro League stadiums only Hinchliffe Stadium in Paterson, New Jersey and Rickwood Field in Birmingham, Alabama were in use longer than Hamtramck.
Michigan has some puzzling names, in that the historic contexts of their origins have been lost to most people today. Hamtramck, more than most American communities, reflects dominating effects of immigration and displacement of native people. [Below: Site marker installed August 2014.]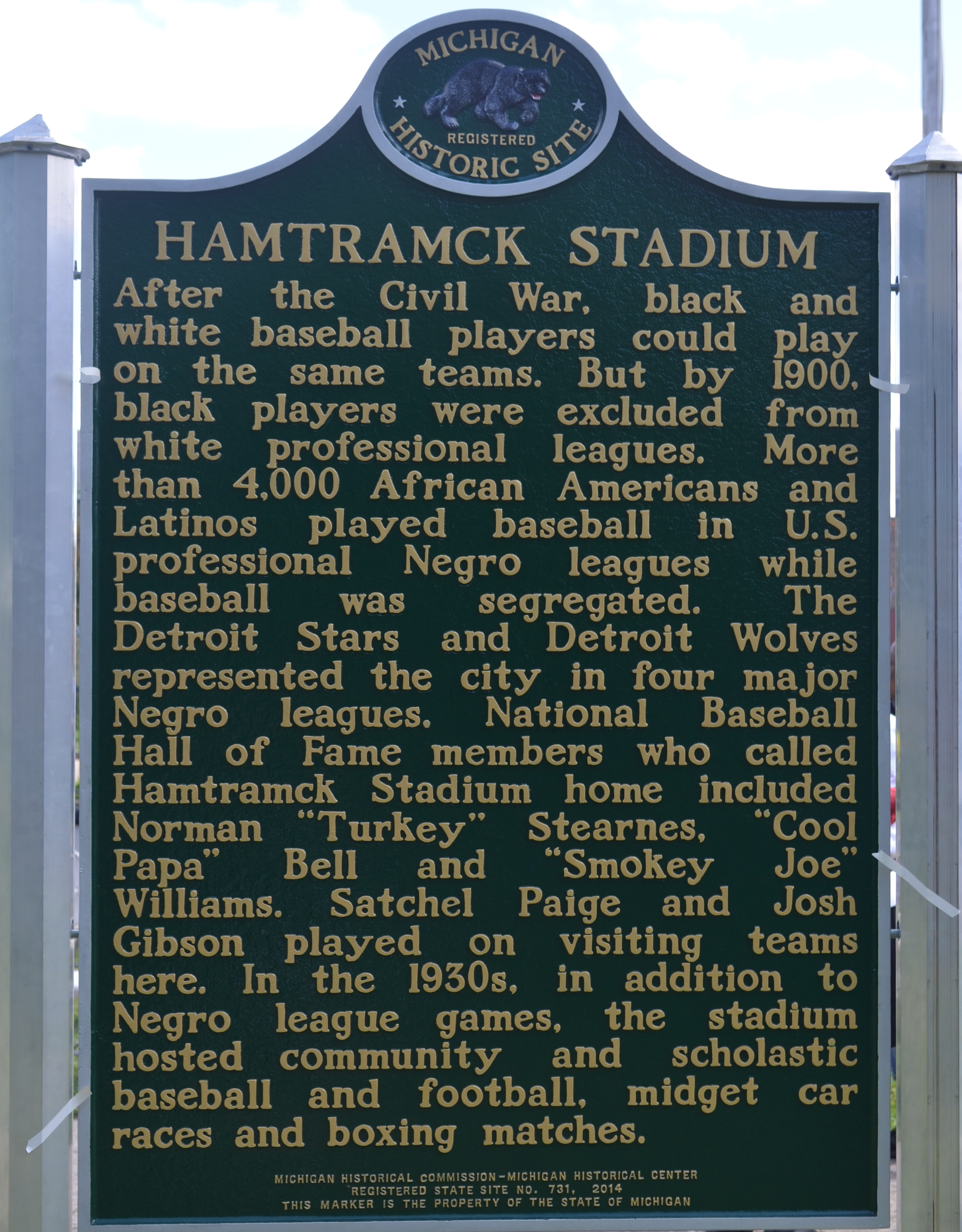
Three.
Hamtramck, a tiny city surrounded by Detroit, had little commonality with Ann Arbor, only 44 miles away, in that spring of 1930 when the University of Michigan Medical School was reeling from the firing of Hugh Cabot in February as dean and chief of surgery. No dean would replace him for three years and the school’s executive committee assumed the role of dean. Frederick Coller was named chair of surgery and appointed Reed Nesbit as the head of urology, but he was a “head” with a single deputy. It’s unlikely that Nesbit and the University of Michigan community knew much about Hamtramck Stadium when it opened that May 1930, although Nesbit became a devoted fan of the Detroit Tigers and certainly knew the name, Ty Cobb. Hamtramck Stadium would become one of the important Negro League venues and is listed on the National Register of Historic Places. [Below: Col. John Francis Hamtramck takes possession of Fort Lernout, part of mural at Detroit Water Building. Wikipedia.]
Jean-Francois Hamtramck (1756-1803), a French-Canadian soldier born in Montreal, came south to join the Continental Army and became a decorated officer in the Revolutionary War. He then served in the Northwest Indian War, displacing native American communities, and was the first commandant of Fort Wayne (Indiana). In 1796 he transferred to Fort Lernoult and the settlement of Detroit, where he died seven years later.
The Jay Treaty, designed by Alexander Hamilton and negotiated by John Jay in 1794, had ceded the fort from Britain to the United States effective 1796, when Col. Hamtramck moved there with 300 troops. Britain reclaimed the fort, by then named Fort Detroit, in the War of 1812. After the Battle of Lake Erie, the fort was returned to the U.S. and renamed Fort Shelby. In the aftermath of this and the Northwest Ordinance Act, territorial judge Augustus Woodward came to Detroit from Virginia with radical ideas on education that he deployed in the University of Michigania in 1817.
The town within Detroit that took Hamtramck’s name began as a farming community of German immigrants and incorporated as a village in 1901. There, the burgeoning Detroit Stove Works attracted industrial workers and shifted the demography from rural farmers to immigrant urban factory workers. By 1910 the Dodge Main Assembly Plant dominated the town, attracting new immigrants and within 20 years the town became heavily Polish and middle class. Of the thousands of factory workers in the 1920s, nearly 80% owned or were buying their own homes. Attracting a new generation of different immigrants, the town (2 square miles and 23,000 people) is now the most densely-populated and most ethnically diverse in the state and in 2015 became the first in the United States to elect a Muslim-majority city council.
Four.
Lessons of history. Each season brings particular infectious risks and in those days when Ty Cobb threw out that opening pitch at Hamtramck 90 years ago, parents were anxious about the summertime threat of polio to their children. Much less commonly, “infantile paralysis” also affected adults and such a victim, it was widely believed, was Mr. Franklin D. Roosevelt, a successful politician when it struck him in 1921 at age 39. He spent years in recuperation, and even afterward continued to struggle with the sequelae of severe lower extremity weakness, that he masked from the public when re-entering the political world as Governor of New York in 1928 and ascending to presidency in 1933. In retrospect, it is more likely that Guillain-Barre was the cause of his neuropathy. The polio story would intersect with the University of Michigan story two decades later. [Below: Photo: Two early-1950s March of Dimes “Fight Infantile Paralysis” posters designed by artist John Falter (of Falls City, Nebraska). (History Nebraska 10645-1197, 10645-4333)]

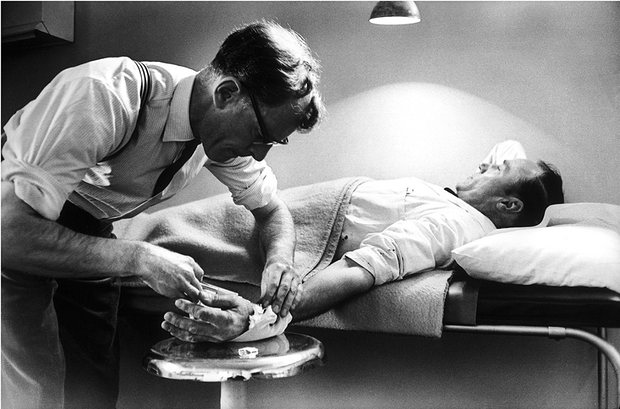
In the summer of 1953, many children throughout the northern hemisphere contracted polio, a seasonal fear of parents. Two children of a UM faculty member in the Surgery Department and practitioner at St. Joe’s were among those diagnosed. They were hospitalized for three weeks in the old “Contagious Hospital” during the presumed infectious period and then transferred, when afebrile, to a large ward of 32 beds in University Hospital (Old Main) on 10 West for the next five months of complete bed rest wearing knee-high boots, to prevent contractions, 24 hours a day.
One of the children, our colleague Skip Campbell, recalls watching Medical Sciences I Building being built from the ground up as he lay in bed. The “Sister Kenney Treatment” involved hot steaming under wool blankets twice daily. Both Campbell children recovered, although Skip’s sister had a life-long limp due to unilateral muscle atrophy. Skip recalled: “Quite a few kids in that place died, including a little girl in our room. Remarkably, I don’t remember a single nurse, doctor or my parents wearing mask!” [Personal recollection, Darrell Campbell, Jr., May 1, 2020.]
Sister Elizabeth Kenney (1880-1952) was a self-trained Australian nurse. After experience in WWI and with the 1918 influenza epidemic who in 1942 opened a clinic in Brisbane where she utilized heat packs and exercise among other regimens for polio. She brought her ideas to the US and settled in Minneapolis where the city gave her a house and she taught and practiced for 11 years. That work would lead into a new field variously called Rehabilitation Medicine, Physical Therapy, and Physiotherapy. [Below, Nurse Kenney, August 4, 1915 enroute to service in the Great War. Wikipedia, John Oxley Library, State Library of Queensland.]

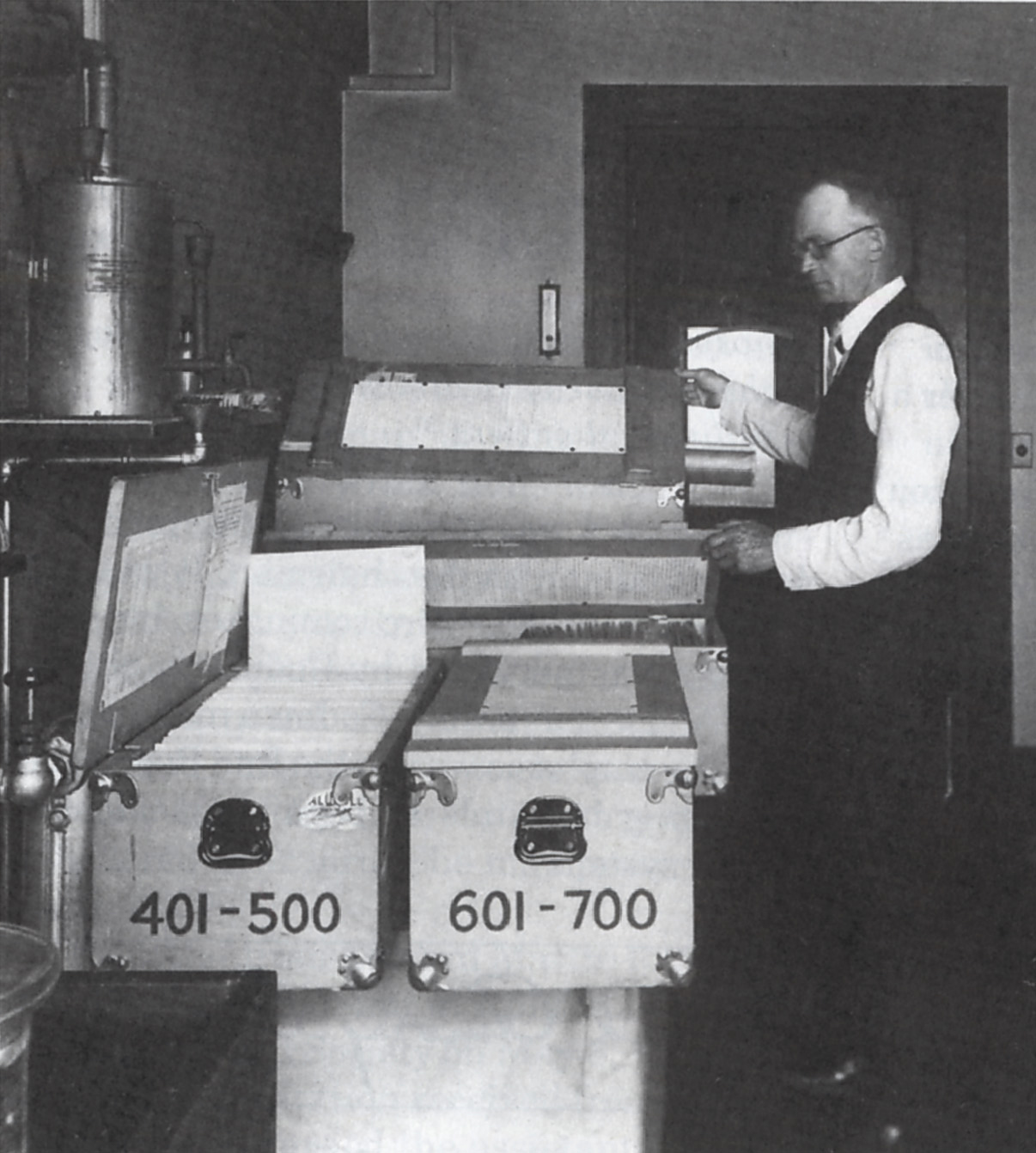
The Salk vaccine and enormous clinical trial (largely funded by FDR’s March of Dimes) coordinated by his professor Thomas Francis at the University of Michigan in 1954 largely eliminated the risk and fear of polio in North America. Salk used “killed virus” in his vaccine and despite safety testing, some batches from Cuter Laboratories contained live virus later linked to over 250 cases of iatrogenic polio. Greater government oversight of vaccine production was called for, but ultimately an oral vaccine from Albert Sabin’s team proved safer and gave more lasting immunity, although U.S. authorities were not initially interested in anything but the Salk series of injections and Sabin had to conduct his first large scale trial in the Soviet Union in 1959. [Below: Photo: Nebraska clinical trial of the Salk polio vaccine, May 1954. From KOLN/KGIN-TV, Lincoln and Grand Island. (History Nebraska RG809-51)]
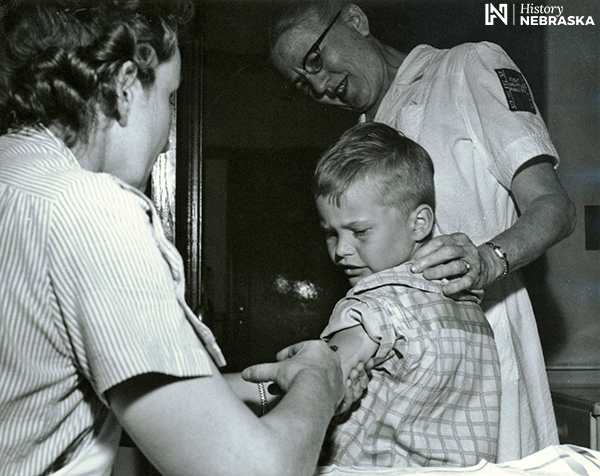
Polio testing children, May, 1954.
Five.![]()
Shimomura Crossing the Delaware, a provocative self-portrait of the artist Roger Shimomura, is prominently displayed at the National Portrait Gallery in Washington DC, – a wonderful place to visit when museums open to the public again.
At first glance Shimomura seems to turn history upside down, but with a little contemplation his work amplifies the idea of the American Dream. The artist fairly claims that America is his country too in 2010 as much as it was that of George Washington, who is more traditionally envisioned crossing the Delaware River on December 25, 1776. Shimomura’s large and striking painting, created nearly 70 years after Executive Order 9066, recapitulates the 1851 work of Emanuel Leutze at the Metropolitan Museum of Art (Washington Crossing the Delaware), but replaces Washington with Shimomura, the colonial troops with samurai warriors, and the geographical location with San Francisco Harbor and Angel Island, once a processing point for Asian immigrants.
In 1942, Shimomura, was not quite three years old when he and his family were forcibly relocated from their home in Seattle to an internment camp in Idaho. Franklin Roosevelt’s Executive Order 9066, signed two months after Pearl Harbor, caused this horrible trauma. That single presidential action designated military commanders to designate exclusion zones from which any American citizens or non-citizens could be excluded and relocated. Census data helped compile lists of such persons. Ultimately, 120,000 people, around two-thirds being U.S. citizens, were relocated to around 50 internment camps.
Ultimately, it is clear that the executive order and resulting program were based on “willful historical inaccuracies and intentional falsehoods,” according to a 1942 Naval Intelligence report that was suppressed by Roosevelt’s solicitor general Charles Fahey. The relocated people had posed no security threat, it was evident even at the time. Fear and ethnic bias left this terrible blemish on Roosevelt’s administration and the American narrative.
The point here is that each of us creates their own origin story from their history as they know it – built on individual identities, beliefs, and aspirations. George Washington and Roger Shimomura had theirs, you and I have ours, and George Floyd had his. Each is as remarkably different as they are similar, sharing remarkable fundamentalities. John F. Kennedy may have said it best in his speech at The American University, Washington, D.C., June 10, 1963: “For in the final analysis, our most basic common link is that we all inhabit this small planet, we all breathe the same air, we all cherish our children’s future, and we are all mortal.”
Postscripts.
Another Shimomura.
Osamu Shimomura (1928-2018) is a name that rings a bell for biological scientists. Not directly related to the American painter, Osamu was born near Kyoto he was a 17-year-old living in the Nagasaki area when the atomic bomb exploded 25 km away, blinding him for about 30 seconds and then drenching him with the black rain of the fallout. Against the odds he survived, was educated, and achieved great academic success, culminating in a Nobel Prize in chemistry in 2008 for his discovery of aequorin and green fluorescent protein.
Ed Tank reminiscences.
Sherman Silber: “I am very sorry to hear of Ed Tank’s passing. He taught me a lot from gender assignment in intersex cases to high diversion with pediatric hydronephrosis, which got me in deep trouble with some very opinionated and obstinate people. He taught me a lot about adrenogenital and testicular feminization, and the bigger issue of the origin of gender identity and SEX preference.”
Paul DeRidder: “I just read your latest “Matula Thoughts” and saw the article on Ed Tank. In my senior year of medical school, 1971, I took a rotation in Urology. Ed Tank was more or less my mentor. I remember him well. He was a determined surgeon, strong personality and great mentor. I remember his suggestion that I review a text in pediatric urology, which I diligently went to the library to review many times. He saw me in the library and was surprised that I was diligent enough to spent time reading the suggested text in my free time at the library. It was because of Ed, my feeling, that I was accepted to the Urology program as an intern, 1972. When I completed my training, Ed had moved to Portland and as I was looking West to set up practice, I contacted Ed and asked if there were any openings in the Portland region. HIs comment was “oh, no it is paradise here and we are saturated with Urologists.” He suggested I look elsewhere. Great guy!”
Thanks for reading Matula Thoughts, this July, 2020.
David A. Bloom