Matula Thoughts
January 1, 2021
Expectations and Epistolaries
2941 words

One.
Calendar reset. After all the hoopla, brouhaha, and general ruckus, today’s customary greeting “Happy New Year” looks ahead with optimism. Human nature, on the other hand, nudges us to also look backward with caution, Janus-like. One year ago, few people expected 2020 would be dominated by a tiny RNA virus. Clues were present but, even without those signals and others soon following, common sense alone should have kept us, vulnerable species that we are, on guard for recurring global pandemics, the last massive one having been only a century ago. [Above: Janus, Wikipedia, source Vatican.]
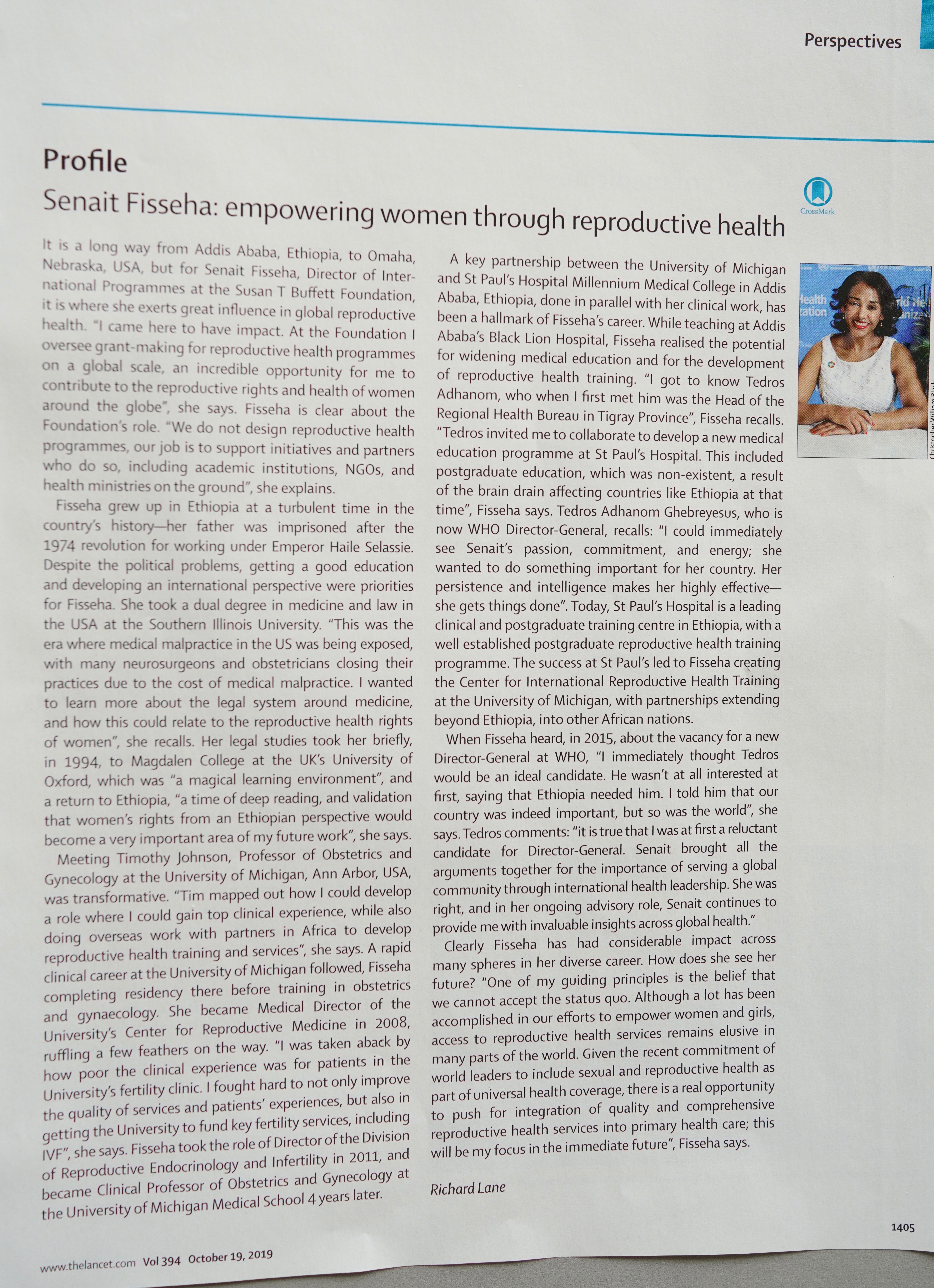
Some argue that the present pandemic is more accurately described as a syndemic: an unfortunate coincidence of a global infectious disease and a range of noncontagious comorbidities. The term came from medical anthropologist Merrill Singer in the 1990s, referring specifically to the interactions among substance abuse, violence, and AIDS (SAVA). Syndemic now denotes occurrences of multiple categories of disease interacting in specific populations. The Lancet expanded the concept for a new series in the journal beginning in 2017. [The Lancet, 389:881, 2017.] A Lancet article this autumn discussed the syndemic nature of COVID-19 in India and the dangers of false optimism as restrictions were lifted there in June. [The Lancet, 396:867, 2020.] In syndemic terms the COVID-19 situation is an acute respiratory viral condition interacting with an array of noncommunicable diseases (NCDs) that tend to cluster within social groups. The key operative words here are respiratory viral infection and social groups (social translates to behavioral, economic and caste). DOI:https://doi.org/10.1016/S0140-6736(20)32000-6
It is beyond ironic that, when the worldwide COVID deaths reached one million by the end of September last year, the United States accounted for 20% of fatalities although representing only 4.25% of the world’s population and arguably possessing much of the world’s best resources to contain the virus. Lacking in this country were national leadership, public trust, and the good will and sense of its people to take sensible measures to minimize spread of a somewhat fragile and moderately contagious virus, SARS-CoV-2.
Two.
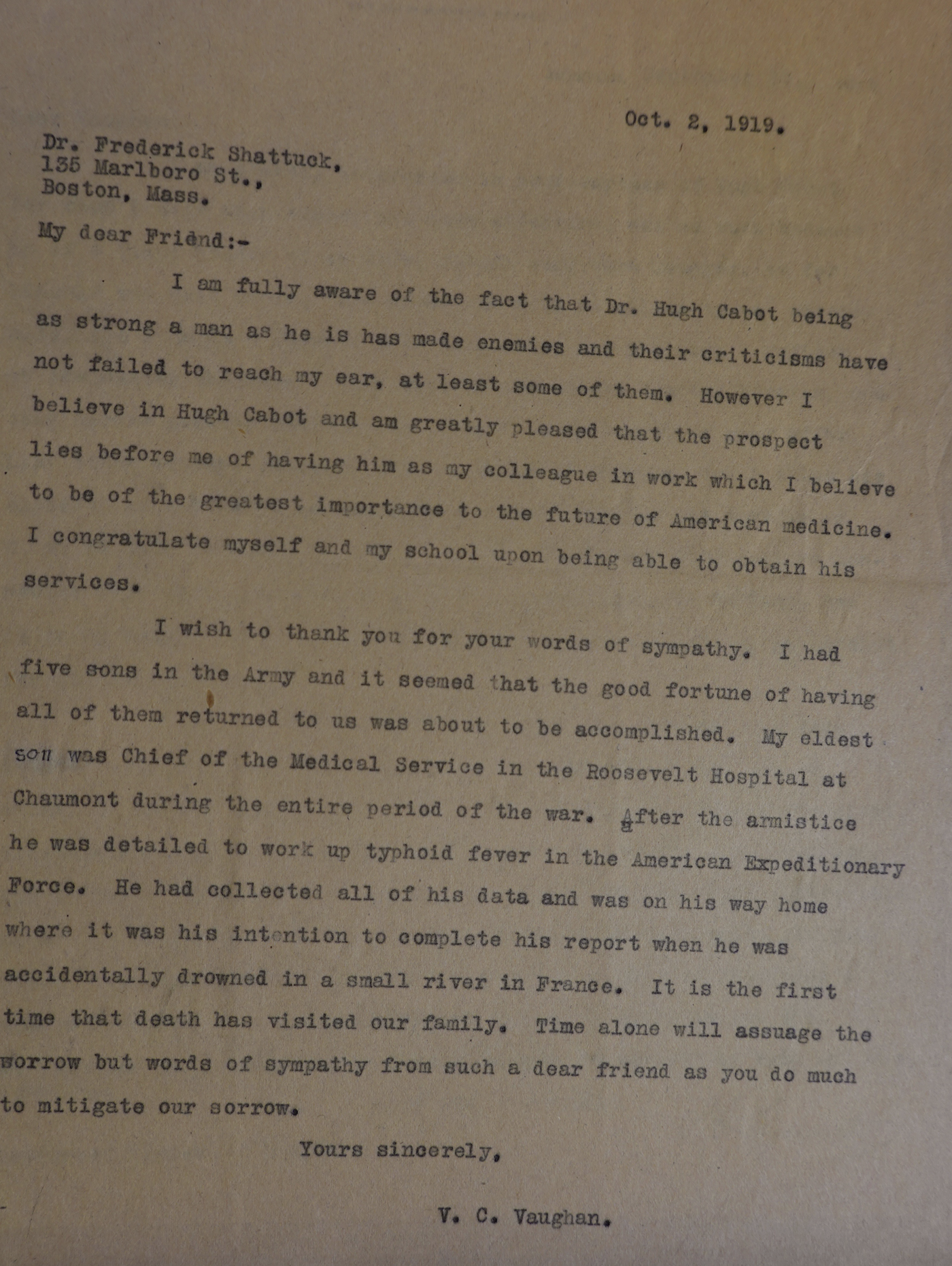
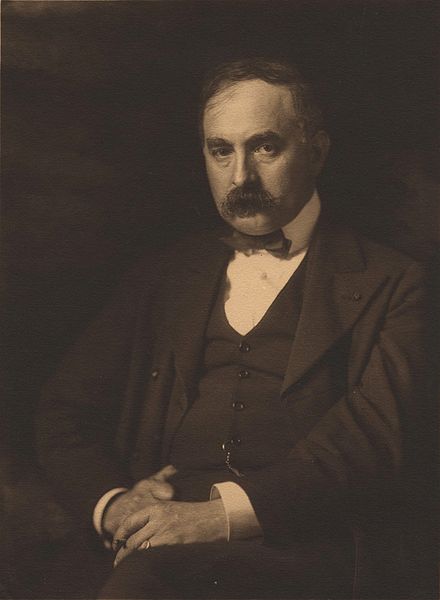
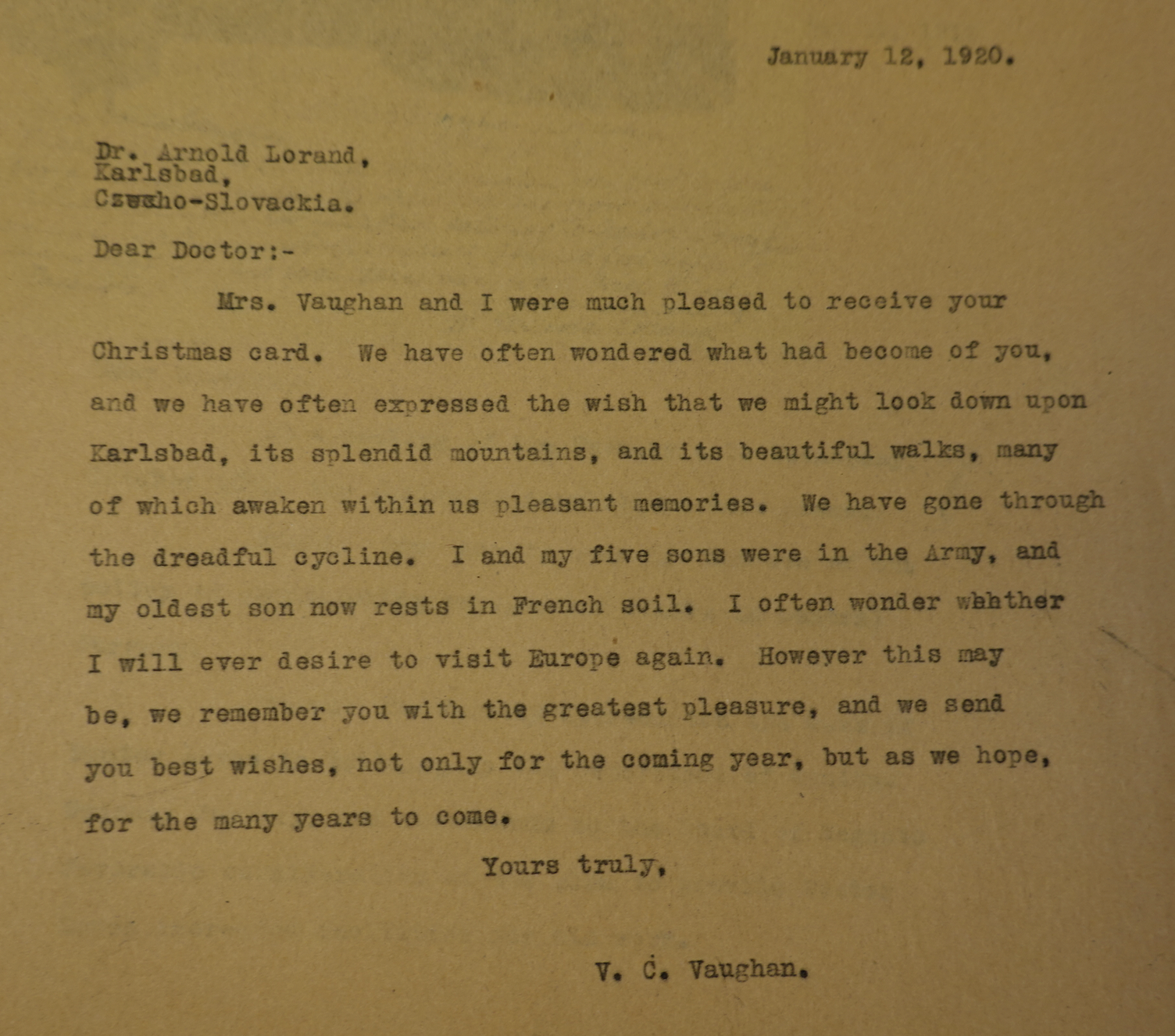
Expectations. History shows that uncertainty about what a new year will bring is nothing new. New years bring gains, losses, and some recoveries as I’ve seen while researching the story of Michigan Urology with far more discovered than two books and Matula Thoughts could contain. One letter found in the Bentley Library fits this January essay nicely: a note sent by UM Medical School Dean Victor Vaughan to his friend Dr. Arnold Lorand in Karlsbad, Czecho-Slovackia, written January 12, 1920. The two friends had lost touch during the terrible war that disrupted their lives, as it had millions of others. They were lucky to reconnect.
“Dear Doctor:-
Mrs. Vaughan and I were much pleased to receive your Christmas card. We have often wondered what had become of you, and we have often expressed the wish that we might look down upon Karlsbad, its splendid mountains, and its beautiful walks, many of which awaken in us pleasant memories. We have gone through the dreadful cycline [‘cyclone’], I and my five sons were in the Army, and my oldest son now rests in French soil. I often wonder whether I will ever desire to visit Europe again. However this may be, we remember you with the greatest pleasure, and we send you best wishes, not only for the coming year, but as we hope, for the many years to come. Yours truly, V.C. Vaughan.”
Lorand (1865-1943) was a physician at the Carlsbad Spa, longevity researcher, and pioneer of modern geriatric medicine. His 1911 book, Old Age Deferred, was popular in America and went through a number of printings. [New England Med Gazette, 47:845, 1912.] He was one of many academic friends gained and visited by the Vaughans during their lives, and epistolaries such as Vaughan’s were the common way people kept in touch, taking more time and crafting than today’s phone calls, emails, or texts. [Below: Lorand and 1913 edition of his book.]

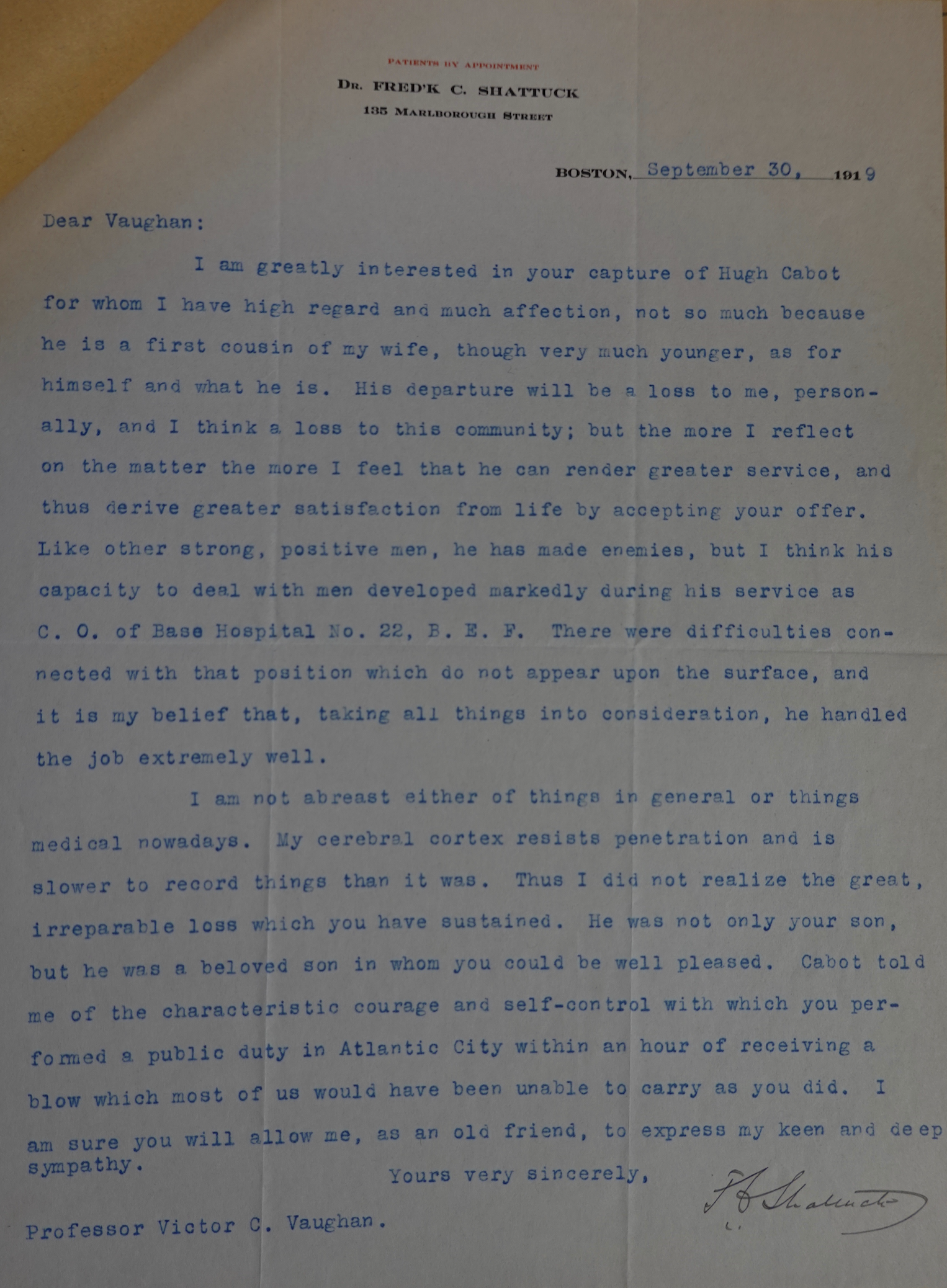
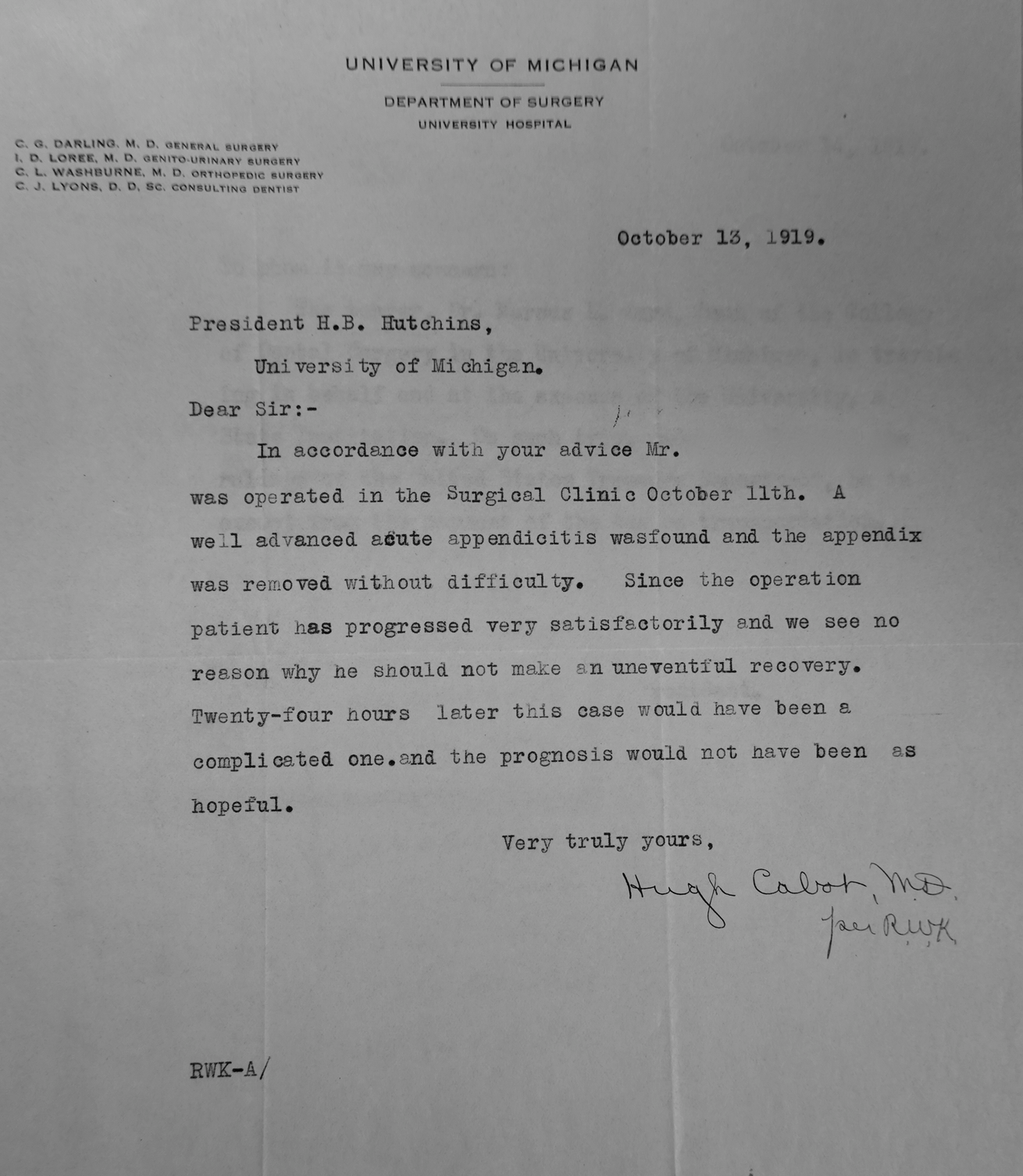
In 1919, with the end of WWI in sight, the Vaughans looked forward to better times as they returned from military duty in Washington, DC to Ann Arbor, but grief followed that summer when their son “Clarence” drowned accidentally while swimming in a river in France, just as troops were drawing down near the end of the war. Dean Vaughan had gotten the news while at the American Medical Association national meeting in Atlantic City in mid-June 1919, just as he was to chair a session. After a few moments to collect himself he stepped onto the stage and took the chair. It was also during this meeting that Vaughan first met Hugh Cabot who had recently returned from more than two years on the Western Front in France serving with the British Expeditionary Forces. Allied Powers and Germany ended their conflict and signed the Treaty of Versailles on June 28, 1919, but within the next 20 years, Germany would break its postwar agreements, subsume Czechoslovakia, and initiate another world war.
After a difficult 1919, the Vaughans hoped for a happier 1920 and the Christmas Card from the Lorands was a happy signal.
Three.
Little things, unnoticed by most people at this first moment of 2021, may become consequential to us in the near future, just as they did last year and every previous new year. The little things may be microorganisms, memes, or people. For example, few in Ann Arbor noticed in January 1933 when Adolph Hitler became chancellor of Germany, although the world soon took note. Many people admired his German patriotism in the dark days after the Treaty of Versailles with his ability to energize domestic industry and get railroads to run on time, but autocratic governance and tyranny never serve a people well and end badly.
In contrast, the 1933 presidential inauguration of Franklin Delano Roosevelt on March 4 was universally noticed throughout Ann Arbor and beyond, marking a turning point in the Depression, although his new administration disturbed many conservative citizens. Where Reed Nesbit stood on this issue can only be imagined as he was not as public with his political beliefs as had been his mentor, Hugh Cabot. Nesbit, however, seemed always to favor the common man.
Roosevelt may not have been a “common man” but his disability brought him close to the myriad daily struggles of common people. Few Americans knew, at this time, that FDR needed assistance to stand and walk, due to polio, it had been believed, incurred in 1921 although a modern view suggests that Guillain-Barré was the more likely cause. [Below: a scene unimaginable in 2021 – Herbert Hoover and Roosevelt together enroute to 1933 inauguration. Library of Congress.]
In retrospect those 1933 transitions began a new chapter in the recurring contest between democratic rule and authoritarian rule, in this instance precipitated largely by the residue of WWI and the Great Depression. Which system best solves a nation’s problems and improves the lives of its people? Hitler exploited his nation with coercion and physical force, while Roosevelt deployed a lucky mix of democratic process, capitalistic enterprise, “New Deal” big government, and moral authority. The public, the press, and academia took far too little notice of this contest until it spilled over into another world war that would give democratic ideas and humanity another reprieve. Cats have a finite number of lives, but we hope democracies have more.
Four.
Annus mirabilis. In January 1971 Jack Lapides began his second year as Section Head of Urology and it was an extraordinary one. As someone who had grown up in Depression times, served in the Pacific in WWII, and seen university and national politics up close, Jack was no “Polly Anna.” Yet, while cautious of threats ahead politically, economically, and globally he relished the opportunities of his new position and robust ideas.
Now, a half century later, it is tempting to try to understand his thoughts as 1971 opened up. Just like today, that New Year began on a Friday. This would be the year Lapides broadcast his ideas on clean intermittent catheterization (CIC) that at the time contradicted medical convention, initially bringing him more ridicule than praise. Nonetheless the concept proved worthy, opening the door to a new era of surgical urinary tract reconstruction and improving the lives of hundreds of thousands of people with urinary tract dysfunction globally. A generation later, leaders like Bernie Churchill in Toronto equated Lapides’s retrograde idea to the most “Nobel Prize worthy concept” in urology.
https://doi.org/10.1016/j.juro.2016.10.080

Lapides (above) published nine papers in 1971 and was appearing on the national center stages of urology regularly just as his predecessors at UM, Hugh Cabot and Reed Nesbit had in their times. At the American Urological Association (AUA) annual meeting in Chicago, May 16, 1971, Lapides moderated a panel called “What Constitutes a Good Urological Residency,” consisting of Peter L. Scardino of Savannah (father of our friend Peter T. Scardino), Clarence Hodges of Portland Oregon (trainee of actual Nobel Prize winner Charles Huggins of UM and then the University of Chicago; later mentor of John Barry), Ralph A. Straffon of Cleveland Clinic (trainee of Reed Nesbit), W.V. Tynes of Norfolk, J.J. Buchierre of Rochester MN, and John Hall of Ann Arbor (chief resident at UM).
The UM urology brand was in wide display at the 1971 AUA in Chicago. Notably, the chairman of the Society of Pediatric Urology that year was Ian M. Thompson, formerly from Ann Arbor, but currently chair in Columbia, Missouri. The 1971 AUA Meredith Campbell lecturer, Willard E. Goodwin of UCLA (a friend and supporter of Lapides) spoke on “Some hermaphrodites, pseudohermaphrodites, ambisexuals, and other ambiguous types I have known.” An “Ask the professor” session featured Goodwin and John J. Murphy urology chief at the University of Pennsylvania. Murphy was a 1952 graduate of the Nesbit program. Residents on the podium “grilled” the professors about their training and absorption into the field of urology, and “seemed to have the feeling somehow that they had been misguided in a urologic career.” [AUA Centennial History Vol. 1 p. 58.]
That oddly negative view of those residents was not repeated the following years nor did it seem to indicate a trend. Lapides’s trainees in Ann Arbor harbored nothing less than great respect and admiration for their chief and experiences in Ann Arbor, as based on my recent conversations with many of them. In the summer of 1971 Charles Adams, Sahir Cittan, John Gambee, and the late Ed Tank completed their urology training at UM while Robert Barnett, Thomas Kub, Thomas Newman, Lee Underwood, and Robert Vinson began their three years of residency under Lapides. I began my training at UCLA that summer, falling under Goodwin’s spell and far from ever feeling misguided considered myself lucky to be there. Sadly 1971 was the year that Jack’s wife, Alice, passed away.
Five.
Ups and downs. A half century ago, 1971, was a great year for an ascending Jack Lapides, but it was a tipping point into despair for another UM alumnus who lost faith in his own future, and indeed the future of our species. This individual dropped out of the conventional world and stepped off the so-called grid to a hermit-like existence in a cabin he built in rural Lincoln, Montana, much in the manner of Henry David Thoreau, or so it seemed at first. The modern-day recluse, however, had far darker thoughts, believing that industrial society could not control its own future and would destroy not only our species, but all others and the planet around us. These ideas took over his brain like a virus and led him to believe that the only recourse was to mail bombs to people targeted as symbolic in industrial society. He anonymously delivered at least 16 bombs that maimed and killed a number of people between 1978 and 1995, becoming known and feared as The Unabomber. In 1995 he sent the New York Times a letter promising to suspend his campaign of terrorism if it printed a rambling essay he included, “Industrial Society and its Future.” Meanwhile, a large FBI team at work since 1978 had failed to identify this “Mad Bomber,” until his brother became suspicious enough to supply the critical tip that led to arrest in 1996 and current imprisonment.
That incoherent essay of Ted Kaczynski (UM Mathematics Ph.D. 1967) has been reformulated to a book, Technological Slavery, available on Amazon where it is described blandly.
“Logical, lucid and direct, Technological Slavery is more than an expansion on the ideas set forth by Theodore Kaczynski in Industrial Society and its Future (aka ‘The Manifesto’). It radically reinvigorates and reforms the intellectual foundations of an age-old and resurgent world view: ‘Progress is a myth. Wild nature and humanity (including human freedom, dignity, and autonomy) are fundamentally incompatible with technological growth.”
Kaczynski is now incarcerated at Federal Prison ADX in Florence, Colorado, serving a life sentence for his murderous campaign, and receives no remuneration for the book.
Considering our ineptitude as a species and society in dealing with many existential crises – pandemics, terrorism, extreme weather, earthquakes, environmental deterioration, poverty, food insecurity, economic and social inequality, ongoing regional warfare and destructive geopolitical conflict – it is no huge surprise that a small subset of our 7 billion people become unhinged by reality. To be so certain of belief and driven to terrorize others by mayhem and murder as Kaczynski, however, is clearly far beyond the pale. And others follow, notably Anthony Warner, last week in Nashville. [Below: Pales of settlement; Ireland 1488 and 1901 Poland and Russia. Wikipedia.]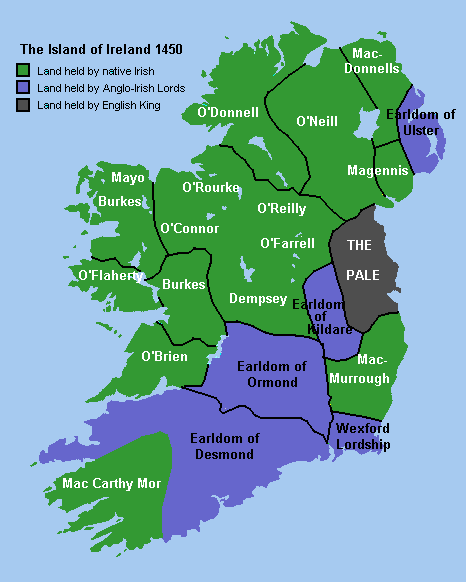

Surely there are myriad constructive ways to build better futures for ourselves and the planet, although we’d better find them more quickly as the opportunities are slipping away.
No one can fully know what 2021 will bring, but we can predict some things will be lost this year: for a start – certainly much glacial ice and rain forest, and likely some essential species. Whatever other critical events we ignore at our peril – time will tell.
Postscripts.
Letters to self. We sent What’s New by email for 20 years and continue to publish the web version, Matula Thoughts, on the internet (maulathoughts.org) on the first Friday of each month.
What’s New, the communication, began in Allen Lichter’s Dean’s Office of UM Medical School in 2001. Some in the office then believed that “we can’t communicate too much” whereas others felt burned-out from the daily barrage of “Too Much Information” on physical and electronic desktops. The idea of producing something predictable but not too frequent, while interesting (one hoped) and reasonably concise, seemed preferable to random uncurated attachments and messages. We began What’s New then at predictable monthly intervals (first Fridays) to provide a finite “weekend read,” of around 15 minutes. The essay transitioned to the Urology Department in 2007 with the web version (easier to access and manage if “followed” on the website) in 2013 as matulathoughts.org making this number 95.
The Dean’s Office of Faculty Affairs, now in the capable hands of Brian Zink, and the Department of Urology, under the excellent stewardship of Ganesh Palapattu, are creating their own modes of communication to fit their new times. Matula Thoughts continues a monthly cadence of essays relating loosely to medicine, Michigan, urology, biology, or other matters in the cabinet of curiosities, from a professor making the final round of bases in the game of academic medicine. This year seems a good time to free up people’s email and liberate many from an unwanted monthly weekend assignment, so we will discontinue the email distribution of What’s New. We will, however, continue the web format Matula Thoughts, that can be accessed by the click of a button on the web site, providing a monthly email and link to matulathoughts.org.
Trees fall in forests.

Why write these essays? The essayist Michel de Montaigne (1533-1592) was an initial inspiration and exemplary modern expressions of the urge to communicate in writing are flourishing. Even if few people in the forest witness the falling tree of an essay, it serves a primal purpose. [Above: Hartwick Pines State Park, Grayling, Michigan, September 2020.]
Comparing the essay form to the nearly-obsolete hand-written letter, the author Claire Messud commented:
“The review and the essay remain a more public, yet ideally still intimate, version of the epistolary. Not a place to share one’s private details, to be sure, but certainly to try to communicate, as precisely and with as much complexity as possible, one’s experience of a work of art, or the evolution of one’s thought….” [C. Messud, Kant’s Little Prussian Head & Other Reasons Why I Write. W.W. Norton, NY, 2020, p. xx.]
A letter assumes an audience, usually of one, although not necessarily of anyone. The act of writing provides a measure of satisfaction and deliverance (of an observation) even if it is simply a “note to self.” Messud’s book is both “an autobiography in essays,” as it’s self-described, followed by a collection of 16 literary and visual art contemplations, but most importantly, one suspects, it is an extraordinary series of personal notes-to-self that bring clarity to the writer.
Metrics
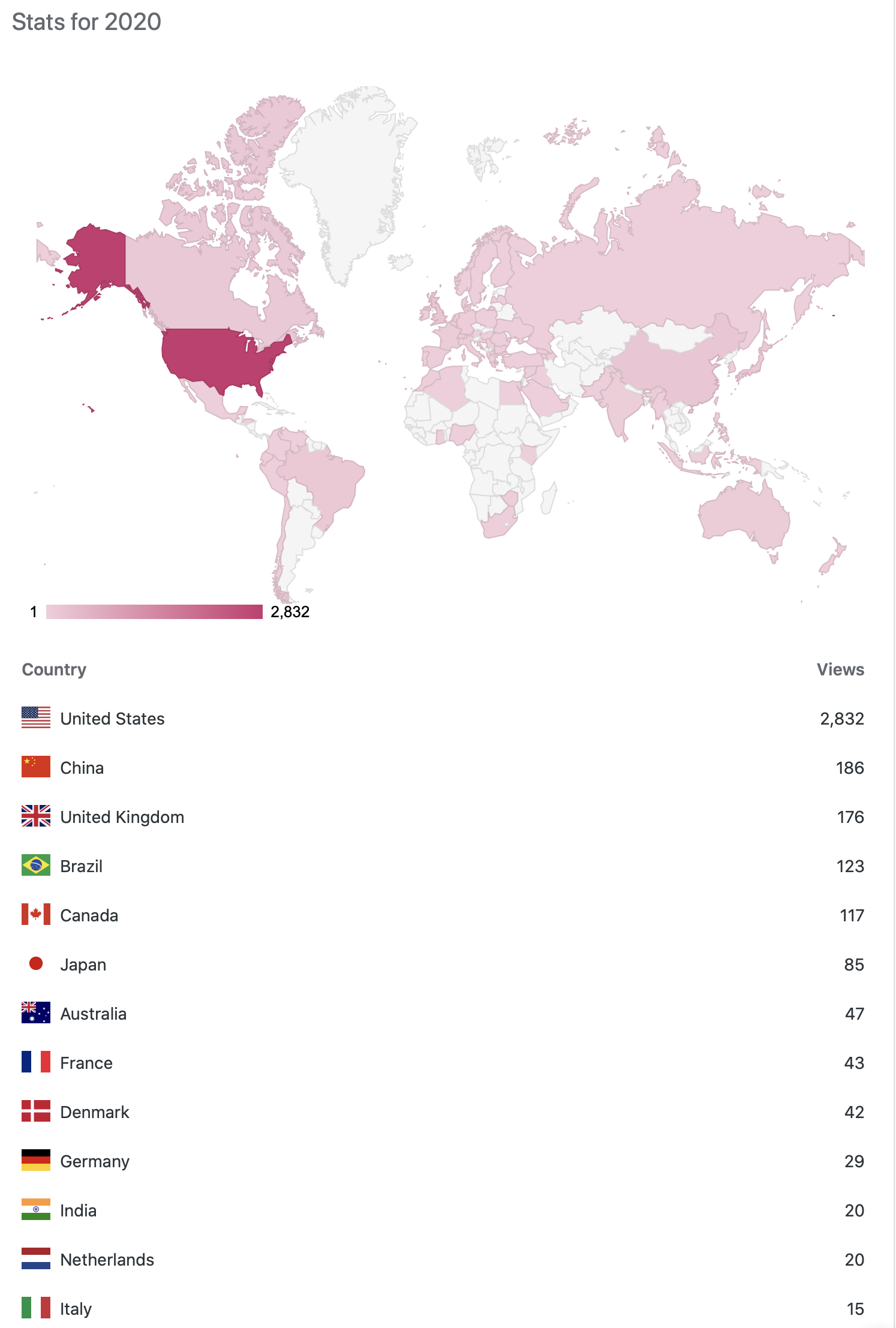
Nothing is beyond the pale on the internet and much of it is measurable. Matula Thoughts took a small dip when the author ceased to be departmental chair of urology at UM in 2019 but readership is back with a rise this year with views at 3458, 3357, and 3929 (31 Dec.) for 2018, 2019, and 2020. This past year 16 countries produced 10 or more “views’ and another 55 countries had “single digit visitors” – enough observers in the cyber forest to justify continuing Matula Thoughts for 2021. Of course, “a view” or “a visitor” is not necessarily a thoughtful reader, but merely a measure of notice within the forest and, happily in terms of forest sustainability, Matula Thoughts doesn’t require many falling trees. Nonetheless, after nearly 20 years of this essay, it remains primarily a “letter-to-self,” if only an affirmation of self that sometimes resonates with someone else. [Below: Word Press readership for Matula Thoughts 2020.]
Thanks for reading Matula Thoughts this January 2021.
David A. Bloom