Matula Thoughts
December 4, 2020
Change and hope
2810 words


One.
Hope. Change and uncertainty are inevitable, but hope is the part of the human tool kit that helps people navigate life’s turbulence. Change may bring hope or horror, as imagined in the fictitious scenario (shown above) of audience response to the novelty of moving pictures in 1895 when the magic of film was an expectation beyond reasonable hope. [Above: “Panic in the Audience when Lumiere Shows his first Film.” Figure from Suddenly this Overview. Peter Fischli and Davis Weiss, Exhibit, Guggenheim Museum, April 2016.]
It is rational to hope that things will return to a semblance of normal after this “final wave” of Covid-19 disrupts workplaces and education, prolongs social isolation, and disturbs belief in science and reason. Humans rebound after bad times and new forms of creativity emerge from calamities, as seen with RNA vaccines. Still, we would do better to remember those bad times and plan for their inevitable return. [Below: Michigan Theater – mostly closed in Covid times and its big screen moving pictures sorely missed.]

Last year just around this time, our department hosted its annual Holiday Party, an event inaugurated by Jim Montie after the Urology Department emerged from a Department of Surgery division 20 years ago. As the department expanded, the get-togethers outgrew Ann Arbor venues and moved to Fox Hills Golf & Banquet Center with the help and generosity of Kathy and Mike Aznavorian. Further growth and blurred administrative boundaries over the years stretched even Fox Hills’s capacity for the UM Urology family, their children, and guests to mingle, see Santa, dine, and dance. A few of our staff put their hearts and souls into planning and deploying the event, with food, avionics for Santa, and gifts for children. When the financial uncertainty of 2008 struck, we hesitated but continued the party. Little did we anticipate an emergent virus from the other side of the planet would break our annual run of holiday parties. Covid not only brings the monetary concern, but also precludes the social interaction and reminds us how much we miss gathering.

[Above: Santa, Holiday Party 2013. Below: Keller and Osawa families, Holiday Party 2015.]

UM Urology has gotten so large and far-flung that hardly any of us knows everyone else – a far cry from my first days here in Ed McGuire’s Section of Urology. With clinical and research activities of our department in at least 15 geographic locations, the challenges of communication and cultural identity are great. Families, organizations, and nations tend to grow far from their roots, straining integrity of the whole. Periodic gatherings can be forms of thanksgivings to recall roots and purpose, restore connectivity, and celebrate diversity. We hope and expect to gather again.
Two.

Origins. With December here, a new year just around the corner, and the second century of urology at UM ahead, thoughts turn to the origin stories that ground our views of the world. Personal origin stories as well as organizational ones are idiosyncratic and complex – and all are rich in certainty, invention, and selective memories. The UM urology narrative, is assembling on our website. [Above: Cropsey painting of early UMMS.]
https://medicine.umich.edu/dept/urology/about-us/our-history/origin-story
Origins are never perfectly clear. The past can never be fully ascertained or known as completely as it actually happened. It can, however, be illuminated and investigated not merely out of curiosity but also to understand options for today, reinforce essential values, and prepare for the future. Our origin stories are lean in the details of the original peoples of the Americas who were displaced by explorers and colonists. Examination of origins forces us to see what’s missing, what’s right, and what’s wrong, thus giving opportunity to improve what’s lacking and what’s incorrect with ourselves and our organizations.
Historians elicit facts, create narratives of the past, and measure it all according to values then and now so as to understand the meanings of those stories. This expansive evaluation is, at first glance, contrary to that of scientists who generally take reductionist approaches that render observations to the simplest explanations. Through methodological analysis scientists may hope to find grander truths in general rules, laws, and theories. Health care providers, ideally, combine the story of a patient (the larger narrative of their past and present) with the facts of observation and clinical investigation.
Three.

Urology is a small detail in history’s medical narrative and its roots at the University of Michigan are uncertain. [Above: medieval uroscopy – man with a matula.] We have no practice logs from UM’s first genitourinary surgeons, Cyrenus Darling and Ira Loree, nor reminiscences to know what they thought of the 1902 “urology” neologism, although they chose not to adopt it. Their recollections of WWI and the Influenza Pandemic can be assumed unpleasant, but how those large events affected their daily lives, families and friends, and political responses can only be vaguely imagined. Who in their time would have thought that the “war-to-end-all-wars” would be followed so quickly by another one and who knew that the 1917 pandemic would end after a third wave in 1920? Who could have doubted that other pandemics wouldn’t follow? Most astonishingly who would dispute, today a century later, that face masks, social distancing, and rudimentary hygiene limit the spread of respiratory infections?
The thoughts of Darling and Loree concerning their replacement in 1919 by “Modern Urologist” Hugh Cabot were not positive and those impressions were exacerbated by his brusque manner, causing their swift departure to the welcoming St. Joseph Mercy Hospital a block away. From this disruptive transition, the UM Section of Urology was born.
No less disruptively ten years later Hugh Cabot, Medical School dean by then, was fired by the regents after losing confidence of the faculty. Reed Nesbit, Cabot’s second trainee, built the Section of Urology from 1930 through 1967, when he retired to Sacramento. Then, after an uncertain six months, Nesbit’s trainee Jack Lapides, was named successor and continued the clinical, educational, and research missions of the Section of Urology from 1968 to 1983. Like Nesbit, Lapides trained a great cohort of urologists of all types, including a great string of pediatric urologists: Norm Hodgson (Nesbit 1958), Tomohiko Koyanagi (N’70 – see Postscript), Ed Tank (N’71), Steve Koff (N’75), Evan Kass (N’76), and Barry Kogan (N’81). Still under the administrative management of the Surgery Department, UM Urology gained Ed McGuire (trained at Yale by Bernie Lytton) as Section Head. This transition, too, caused disruption, with the loss of Ananias Diokno to the Beaumont system.

The five-person Section of Urology under Ed McGuire (above) welcomed me and my family to Ann Arbor in the summer of 1984. The small section of five is now the large Department of Urology of 50 full-time faculty led by Ganesh Palapattu. Our academic space, initially on the fifth floor bridge between the old Mott and old Main University Hospital, moved to the second floor Taubman Building when it opened in 1986, and then the third floor of Taubman in Jim Montie’s early years as Urology Chief. That space underwent a well-needed facelift this autumn. Although this is the administrative hub of the department, our faculty have offices in the Cancer Center, North Ingalls Building (the old St. Joes Hospital), North Campus Research Complex (our Dow Division of Health Services Research in the old Pfizer Research campus), Muskegon’s West Shore Urology, and clinical and surgical activities at more than a dozen other sites.

[Above: Taubman Administrative Urology. Sept. 15, 2020. Below: September 30, 2020.]

The challenges of this Covid year are not over, as we yearn for a return to social proximity and in-person conferences. The postponement of the yearly Nesbit Alumni Meeting, along with other regular medical and scientific sessions was disappointing, but not unprecedented. The AUA, for example, also cancelled this year as well as in 1918, 1919, 1943, and 1945.
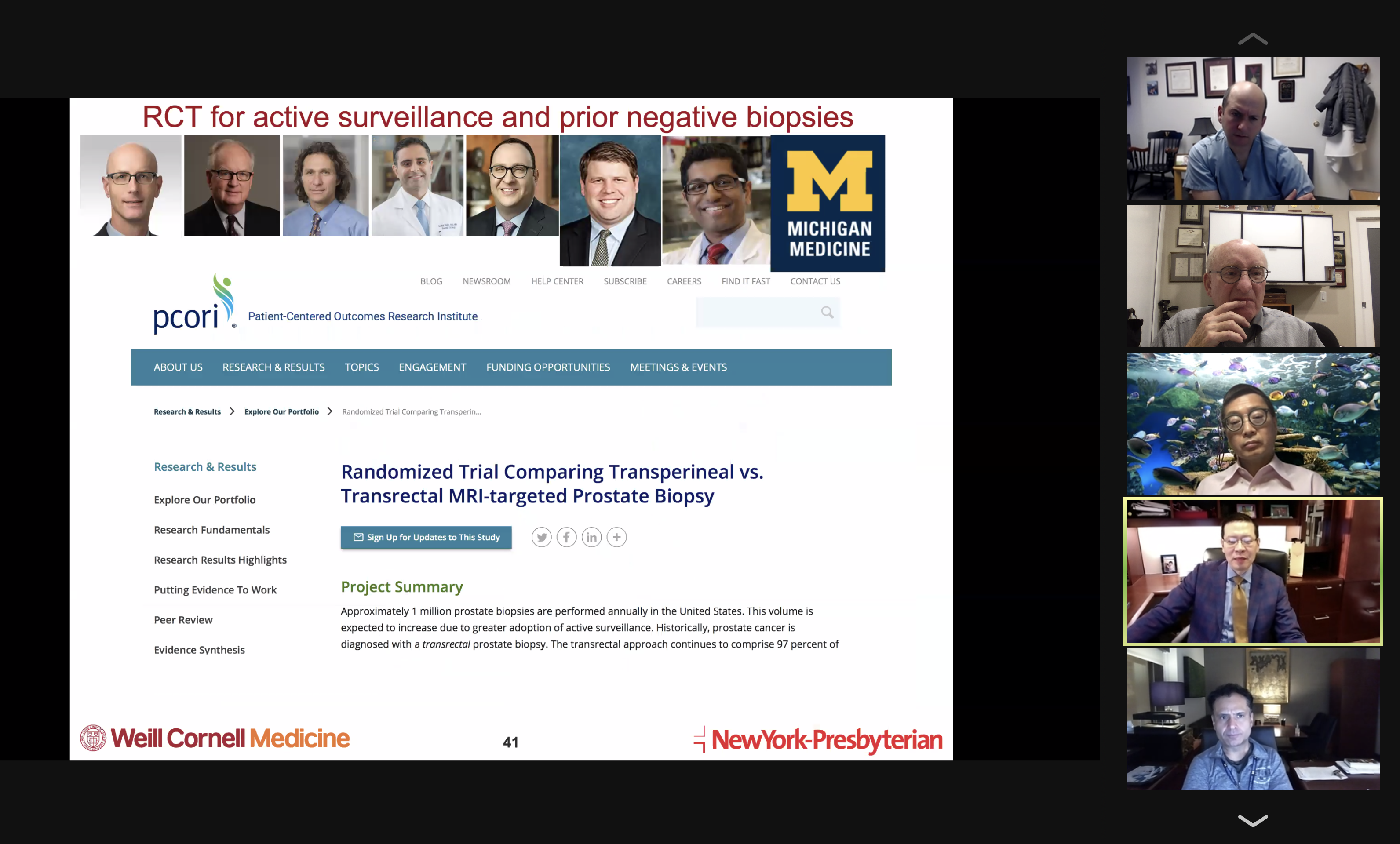
Academic routines are changing into new normals, such as our zoom visiting professor lecture in mid-November from Jim Hu at Cornell, shown below in one of his slides. Still, we miss our conference rooms.
Four.
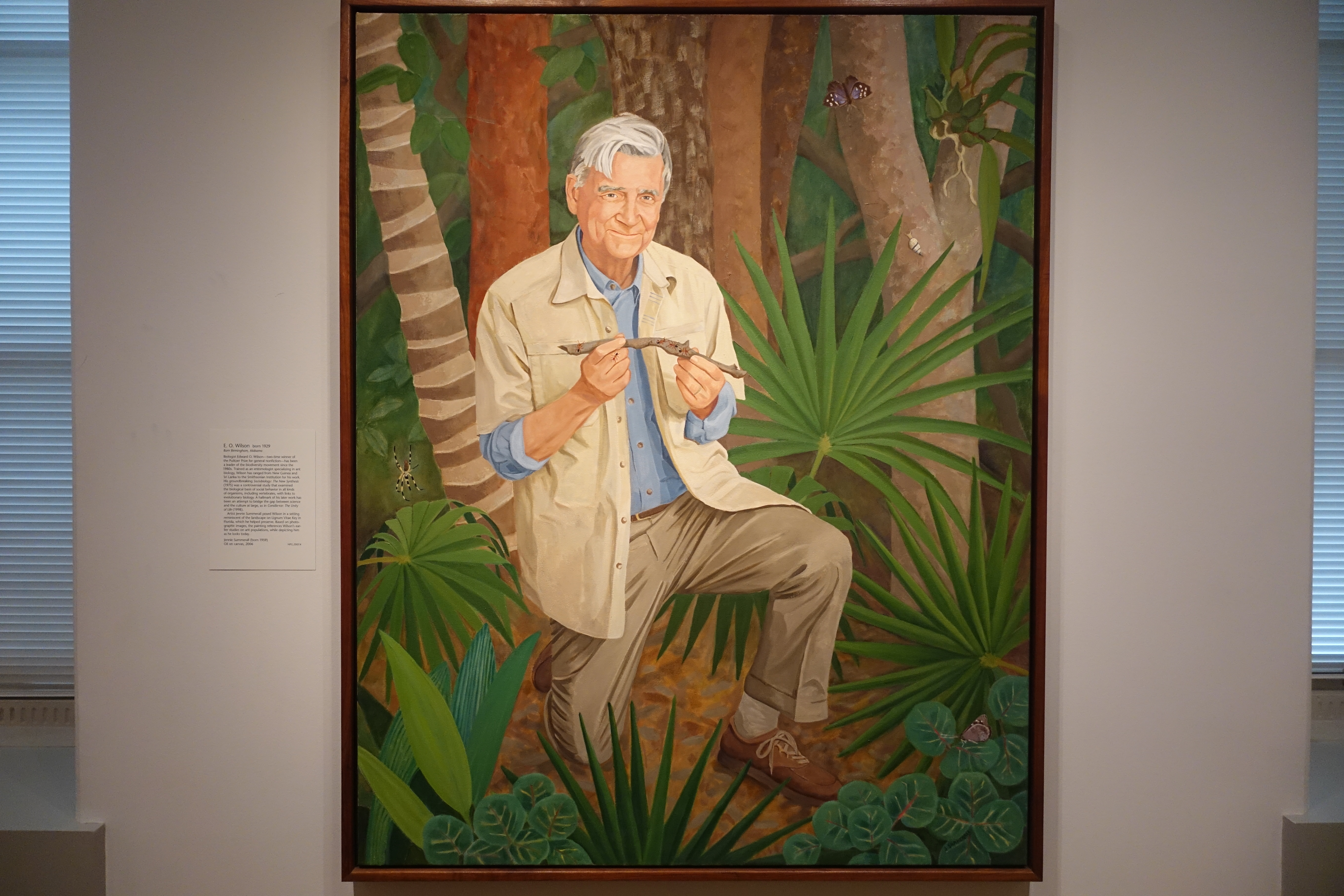
Narratives. The writing process for the UM urology story has strengthened my admiration of others far better at that art. My career, not primarily one of writing, was directed to what Hippocrates narrowly considered “the art of lithotomy,” but grew into its surgical cousins of orchidopexy, hypospadias repair, pyeloplasty, bladder reconstruction, and other needs of modern urology. Turning facts into authentic narratives is a different occupation and certain writers stand out: John McPhee and E.O. Wilson for nonfiction, or Kazuo Ishiguro and David Mitchell for fictional story-telling. McPhee at age 89 continues to weave artful narratives of fact and people, while Wilson at 91 explains science with clarity and grace. Mitchell at 51 creates tapestries of fact and imagination, crossing fictional genres. Nobelist Ishiguro, at 65, writes novels that explore the uncertainty of memory and its deceptions. The authenticity of great fiction is a mirror to reality; as the Good Lord Bird miniseries proclaims: “All of this is true, most of it happened.”
Our parochial story, The First Century of Urology at UM, is an accounting of real people and events that built a small specialty in a great public university amidst the contexts of its times, providing and creating state-of-the-art clinical care (such as it was), generating new ideas, educating successors, and leading colleagues.
We were fairly certain of the sequence of Nesbit’s early trainees and associates in our Origin Story of Urology at UM, but new information kept popping up. For example, Susan Dorr Goold, daughter of our recently deceased colleague Dick Dorr (Nesbit 1968), gave me pictures from her dad’s office but the identity of one drew a blank. Skip Campbell and Mac Whitehouse identified the photo as Rigdon “Rod” Ratliff, (Transylvania College A.B. 1924, UMMS 1929) who practiced urology at St. Joe’s. In medical school Ratliff became interested in surgery and urology under Cabot and Coller, and was likely influenced by Huggins and Nesbit – trainees and later junior staff under Cabot. With his MD in hand, Ratliff went across the street for internship at St. Joe’s and fell under the influence of Ira D. Loree, the UM genitourinary surgeon displaced nearly a decade earlier by Cabot. The cataclysmic stock market crash a few months into internship undoubtedly shaped Ratliff’s career plans and he remained at St. Joe’s in practice with Loree, the early years serving as a de facto residency in urology.
By 1935 Ratliff was considered a legitimate urologist and Nesbit appointed him “Instructor in Urology” without salary. Loree died on August 11, 1936 and Ratliff took over his practice, revising his UM title in 1938 to “Part-time Instructor,” allowing more time for St. Joe’s practice. Ratliff maintained this title until 1946. Curiously, Ratliff didn’t join the AUA until 1946, his application endorsed by Nesbit and Robert Breakey, a Lansing urologist. Ratliff continued to teach students and interns, and one of them, Tom Newman (Nesbit alumnus 1974 – now retired in Tucson), recalls Ratliff teaching him the “Water sink window test.”

Ratliff (above) collected urine samples in clear specimen bottles (modern matulas) before cystoscopy, holding them up to the window by the sink in the cystoscopy suite and if clear to daylight he poured the urine into the sink and completed the cystoscopy. Only if turbid, would he send the specimen for urinalysis, culture, and sensitivity. At University Hospital, however, Newman discovered a very different approach; Lapides insisted on routinely spinning the urine and staining it with methylene blue before examination under the microscope and then dipstick urinalysis, with culture and sensitivity, if necessary. One approach was practical and cost effective, the other was richly academic. Newman fondly recalls Rigdon as a quiet gentleman. Clearly, Dick Dorr shared that admiration. Ratliff retired in December, 1973, according to the AUA files (found for us by Tupper Stevens) transitioning his AUA status from active member at $75 per year to senior member at $15. At home on 231 Corrie Road in Barton Hills, Ratliff died of a heart attack January 29, 1977. He was the last link between Hugh Cabot’s era and ours.
Five.
The uncertainty of history. This turbulent political season, a friend referred me to the recent book, American Dialogue, by American historian, Joseph Ellis, who explained a central irony in his field.
“There is an inconvenient truth that most historians acknowledge under their breath, admitting that objectivity, in the sense that mathematicians or physicists, use the term, is not a realistic goal for historians. The best they can strive for is some measure of detachment, which serves the useful purpose of stigmatizing the most flagrant forms of ideological prejudice (i.e. cherry-picking the evidence to claim that Thomas Jefferson was an ideological Christian or Andrew Jackson was a New Deal Democrat). But as you believe that the study of history is an ongoing conversation between past and present, detachment itself is delusional. In his Style in History (1974) Peter Gay put the point succinctly: ‘History is always unfinished in the sense that the future always uses the past in new ways.’ In fact, the past is not history, but a much vaster region of the dead, gone, unknowable or forgotten. History is what we choose to remember, and we have no alternative but to do our choosing now.” [Ellis, American Dialogue, 1918. p. 7.]
Certitude, whether moral, intellectual, or political, is a tricky matter as reflected in this column last month when we tried to make a case for an enlightened Certainty 2.0 that allows one to retain some degree of uncertainty to allow for “I’m not so sure” and keep asking questions. Perhaps H.L. Mencken overstated the matter when he claimed that moral certainty should occupy a low rung in the ladder of human intellect, but he had a fair point.
The moral certitude of John Brown, in song, epic poem, or current Showtime series, The Good Lord Bird, epitomizes the smugness of Certainty 1.0. Timothy McVeigh’s ideological certainty terrorized Oklahoma City in 1995, striking against the Federal government by bombing a federal building, killing 168 people and injuring more than 680 others. Similarly, Ted Kaczynski (UM Mathematics Ph.D. 1967), certain that industrial-technological society was subjugating mankind and destroying the planet, responded by sending bombs to university faculty and airlines in 1978, to “get back at the system.” He wreaked havoc on the lives of random people who represented modern society or happened to be in the way of the bomb. This campaign precipitated a long FBI investigation that ended with arrest in 1996 (see Wikipedia). Religious certitude (perhaps a form of ideological certainty) fueled the destruction of the World Trade Center on September 11, 2001.
Self-serving certitude, another broad form of certainty, is that of psychopaths who justify their actions by personal convenience, often framed by occupation or paycheck, as mentioned here last month, with attribution to H.L. Mencken, Lewis Sinclair, C.E. M. Joad, and others: “It is difficult to get a man to understand something, when his salary depends on his not understanding it.” Closely related is political certitude, as in recent seasons has tested the flexibility of the American Experiment.
Immaculate Misconceptions, the title of a section of the Law chapter in Ellis’s book includes two extraordinary quotes relevant to certitude and to stimulate your uncertainty as a reader we defer their sources to the postscript.
Source A. “When a case comes to me, I don’t do whatever I feel like doing, I have a standard. That standard is what would the people at the time the Constitution was enacted have said.”
Source B. “Some men look at constitutions with sanctimonious reverence, and deem them, like the ark of the covenant, too sacred to be touched. … We might as well require a man to wear still the coat which fitted him when a boy, as civilized society to remain under the regimen of their barbarous ancestors.”
These ideas relate to the question of the role of originalism or textualism in law. Adjudication of today’s uncertainties according to the exact words of a set of historic bylaws might be considered a cop-out, relieving decision-makers of consideration of contemporary complexities and values. One expects that was not Scalia’s intent in his heart of hearts, but rather his starting point to consideration of legal questions. We surely hope our judges and wise leaders struggle intellectually with uncertainty to arrive at a Certainty 2.0 in their consequential decisions.
Postscript.
Sources. A. Antonin Scalia, speech at the University of Fribourg, March 8, 2008. B. Thomas Jefferson to Simon Kercheval, July 12, 1816. [J. Ellis, American Dialogue, The Founders and Us. Vintage Press, NY, 2018. p. 151.]
The Good Lord Bird, is a 2014 book by James McBride on John Brown and its Showtime dramatic series offers an ironic introductory quote, “All of this is true, most of it happened.” This complements Don Coffey’s enduring admonition to his research students to try to understand the difference between facts and true facts, reminding how certainty is tenuous but some things are deeply true to us.
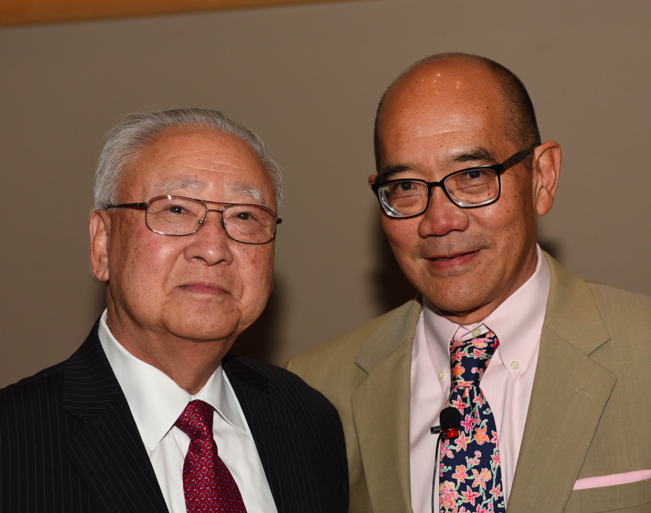
Congratulations. The Japanese Government recently awarded Tomohiko Koyanagi The Order of the Sacred Treasure, Gold Rays with Neck Ribbon in recognition of outstanding contributions to medical education and research. https://en.wikipedia.org/wiki/Order_of_the_Sacred_Treasure

[Above: Tom Koyanagi. Below: Order of Sacred Treasure.]

Thanks for reading Matula Thoughts this December, 2020.
David A. Bloom, University of Michigan Department of Urology