
DAB What’s New March 4, 2016
The March of time, money, & art
3923 words

One. Time flies, but sometimes we have to slow it down. Today would have been March 5, but for a corrective leap year adjustment. This necessity is proof of the slightly imperfect alignment of humans to nature – we meter out our seasons and years with great reliance on lunar and solar cycles, yet our calendars and clocks can’t quite match heavenly reality. Nevertheless, since Robert Hooke’s anchor escape device, human ingenuity has been measuring time with increasing precision. Pocket watches, developed in the 16th century, were the most common personal timekeepers until military trench watches (pocket watches with lugs for a strap) became popular around WWI, proving more practical than a watch in a soldier’s pocket. The wristwatch quickly came into fashion. Today cellphones threaten wristwatches for top position in personal timekeeping, although wrists are contesting the matter with physical activity trackers that also monitor time, pulse, and even messaging alerts. Whether by wrist, phone, or clock most people are compelled to track time at home and at work. In the health care environment time measurement has come to sharply impact patient care and residency education due to intense attention on clinical throughput and duty hour regulations. [The pocket watch shown above is a rare Donald Mozart three-wheel mechanism watch made over 150 years ago.]
Two. Time is money, it is often said. If I need furnace repairs this winter, a repairman will reacquaint me with that fact. This is also true for legal services, cabs, baby sitters, or employees in your business. Ultimately, because most of us are employees for someone or some organization, we each have a personal stake in the belief that time equates to money. Healthcare used to be somewhat different, being a professional service in which the service was valued as a parcel of work rather than a unit of time. A doctor’s visit, for example, was charged as the actual “visit” with the time factor accounted for indirectly. New knowledge and technology added complex services to the toolkit of health care and the relative value unit (RVU) joined the language of medicine. Urethral catheterization, for example, takes less time and expertise than radical cystectomy, a fact now accounted for in the charges or RVUs. The physician work RVU for catheterization (CPT 51702) is 0.5 (although after facility expenses and malpractice expenses are factored in the total RVU grows to 0.87 to 2.0 depending upon whether the work is done in a hospital or an office). For open radical cystectomy with urinary diversion (CPT 51590) the physician’s work RVU will be 36.33 and the total RVU including facility and malpractice expenses will be 55.66. The assignment of an RVU number to robotic cystectomy is under discussion. Radical cystectomy is one of the most technically difficult and risky operative procedures, with significant mortality, morbidity, complex postoperative care, and the highest postoperative readmission rates. In terms of work (preoperative, operative, postoperative, and global exposure) and liability it is easily more than the “equivalent” of 36.33 urethral catheterizations, in my opinion as someone who has performed both procedures. If it is your urethra getting catheterized, of course you want skill, kindness, and attention to the process. Yet, to equate the effort of 36 catheterizations to a single radical cystectomy is like comparing 36 bicycle rides to flying a Boeing 787 or Airbus A380 full of passengers across the Pacific Ocean. Both take skill and both carry some risk, but the differences are enormous. [Data thanks to Malissa Eversole & Irene Gundle]
Just as all procedures are not equal, neither are all clinic visits the same, although less disparity pertains. One new patient visit may be fairly straightforward with discovery of a simple problem defined as ICD-10 code X and perhaps a distinct solution proposed in the form of CPT code Y. If such simplicity had pertained for all my patients and clinics over the years, life would have been easier although less interesting. Some clinic visits are especially challenging, taking deep concentration and probing examinations and conversations that are not always easy. Occasional clinic encounters are excruciating, with unwilling kids, angry parents, painful social circumstances, and no clear solutions. Yet even these complex occasions are gifts of a sort in that they test our mettle and make the other encounters, by contrast, satisfying and sweet.
Most of us understand the need to steward resources, standardize work as much as possible, and create efficiencies to meet payrolls and manage our mission at large. However, a sharp focus on clinical throughput, with standardized 15-minute encounters and checklists that must be obeyed, runs counter to our values, counter to patient satisfaction, and counter to the excellence we espouse. Still, our eyes stray to clocks on the walls, (although it is a mystery why they are so often wrong) or watches on our wrists, the latter being easier to consult unobtrusively than cell phones and are more accurate than those wall clocks.
Three.
 Ben Franklin wrote “time is money” in Advice to a Young Tradesman, written by an old one although the idea has a far older provenance. It is fitting that Ben is featured on our largest circulating currency denomination (since 1969 when larger bills were retired). The Franklin has become the international monetary standard and is worth more than its weight in gold if you figure that the bill weighs around a half a gram and with the price of gold at $1200 per ounce that comes to about $40 per gram or $20 for a Ben Franklin. The US Bureau of Engraving and Printing says that the average C-note remains in circulation about 7.5 years before replacement due to wear and tear. The new bill, with its anti-counterfeiting technology, costs about 12.5 cents to produce, compared to 7.8 cents for the older version (shown above) before 2013. Curiously, and I think dangerously, some people are calling for eliminating this “high” currency note, as humanity seems to be placing its faith in electronic monetary transactions. [Getting rid of big currency notes. NYT Editorial Feb. 22, 2016]
Ben Franklin wrote “time is money” in Advice to a Young Tradesman, written by an old one although the idea has a far older provenance. It is fitting that Ben is featured on our largest circulating currency denomination (since 1969 when larger bills were retired). The Franklin has become the international monetary standard and is worth more than its weight in gold if you figure that the bill weighs around a half a gram and with the price of gold at $1200 per ounce that comes to about $40 per gram or $20 for a Ben Franklin. The US Bureau of Engraving and Printing says that the average C-note remains in circulation about 7.5 years before replacement due to wear and tear. The new bill, with its anti-counterfeiting technology, costs about 12.5 cents to produce, compared to 7.8 cents for the older version (shown above) before 2013. Curiously, and I think dangerously, some people are calling for eliminating this “high” currency note, as humanity seems to be placing its faith in electronic monetary transactions. [Getting rid of big currency notes. NYT Editorial Feb. 22, 2016]
In health care, the concept that time is money applies across all nations and health care systems. In corporate U.S. health care, clinic visits are set in many places at 15 minutes of “face time” with physician, nurse practitioner, or PA. In the NHS of the United Kingdom 10 minutes is a common standard. In third world countries, any such face time might be a rare occasion unless you have cash in hand. Facilities and staff cost money and health care expenses need to be covered by some source, so it seems rational to measure and ration time as well as physical commodities. Facing off against such reality, however, is the nearly universal belief that health care is a natural human right and that its best delivered at the individual level by professions (and, now, teams of professionals).
Time value of money is a financial calculation that dates back to the early days of the School of Salamanca formed by Spanish and Portuguese theologians in northwestern Spain around the first half of the 16th century. (The old city of Salamanca in Castile and León is a UNESCO World Heritage Site.)

Martín de Azpilcueta (1491-1586), pictured above, was an early member of this important school of thought. This Basque canonist and theologian was an innovator of monetarist theory and it was he who allegedly conceptualized the time value of money in the sense that the present value (PV) of a sum of money equals its future value (FV) given a specified rate of return (r) divided by 1 plus r. That is if the Department of Urology gives the University of Michigan Clinical Enterprise $1,000,000 for new capital projects and assumes a rate of return of 7% (the typical interest rate for a savings account in days not so long past) then the FV at 10 years will be $1,700,000, assuming the original sum and the yearly interest returns remain intact. In other words, a million dollars today if invested in those circumstances could be worth 1.7 million dollars in 10 years. Of course, this is not quite as good as that historic savings account at 7% where the interest was compounded annually, in which case the future value at 10 years would be a little over $1,967,000. That is the difference between an annuity and a savings account. Darwinian forces have propelled financial markets to increasingly creative and complex devices, such as credit default swaps that gained recent attention in the film The Big Short, or the more recent contingent convertible bond (CoCo) that exchanges risk for the ability to suspend payment, convert the bond into equity, or write it off totally.
In 1748 Franklin wrote: “Remember that Time is Money. He that can earn Ten Shillings a Day by his Labour, and goes abroad or sits idle one half of that Day, tho’ he spends but Sixpence during his Diversion or Idleness, ought not to reckon That the only Expence; he has really spent, or rather, thrown away Five Shillings besides.” [Courtesy Kate Woodford at Yale University, Papers of Benjamin Franklin Project]
This is the innate paradox of academic medicine: since clinical revenue sustains the enterprise, every part of the day diverted to education, research, and administration is costly, lacking proportionate revenue. Nevertheless, education, research, and their administration are essential to our mission. For a healthy academic clinical department these other parts of the mission consume a minimum of 20% of a clinician’s effort and the ability to support those efforts comes from endowment, institutional support, and the overachievement of clinical faculty in terms of clinical productivity.
Four. As scarce as face-time may be for patients and the professionals who provide it, that time and attention within those moments are polluted by the mandatory processes of electronic health record systems, third party payer requirements, and demands of “meaningful use” documentation. I call your attention once again to the crayon drawing of a doctor’s visit by an 8-year old girl featured on a JAMA cover article in 2012 by Elizabeth Toll and contrast that to any of the many other artistic renderings of this ancient professional service from Renaissance painting to Normal Rockwell. Something seems to have changed. (Interestingly, Rockwell’s family doctor doesn’t seem to be wearing a watch.)

[Above: detail from The Family Doctor by Norman Rockwell 1947; Below: The cost of technology. JAMA 307: 2497, 2012. Elizabeth Toll. © Thomas C. Murphy, MD]

Five. Time piece manufacturing came to Ann Arbor 150 years ago when Donald J. Mozart moved here just after the stockholders of the MoZart Watch Company in Providence, Rhode Island fired him as superintendent. Mozart’s three-wheel watch had proven unsuccessful and the new superintendent replaced Mozart’s design with a conventional movement and renamed the firm the New York Watch Company. Mozart improved his 3-wheel design in Ann Arbor, but was able to produce only about 30 movements before closing up operations four years later in 1870.
He sold the manufacturing equipment to the Rock Island Watch Company for $40,000 cash plus $25,000 in stock and gave away the existing watches to stockholders and friends. One of these was recently sold at auction in NY [Introductory illustration & below: Bonhams Auction 21971 12 June 2014 Lot #1128 A very rare gold filled open face ‘chronometer-lever escapement’ watch Signed Don J. Mozart Patent Dec. 24, 1868. US$ 20,000-25,000].

Mozart was still living in Ann Arbor as of May 14, 1873 when he filed a patent from here, but died four years later in 1877 and was buried at Forest Hill Cemetery (as was Rensis Likert, discussed last month on these pages).
Six. A noteworthy and thoughtful artist, Evelyn Brodzinski, when asked her definition of what constitutes the stuff we call “art” replied, “Art is anything that is choice.” This idea stuck with me and I often quote her at our speaker introductions during the annual Chang Lecture on Art and Medicine each July during the Art Fair. This phrase came to me again when I read Hugh Solomon’s retirement letter this past December. With his retirement, urological manpower loses one of its most excellent physicians and surgeons. Retirement was a difficult decision, Hugh noted, but his timing seemed right: “I have been lucky to have interfaced with so many wonderful people who have taught me the value and sanctity of life. Everyone has a story to tell if you are prepared to listen.”
Stories, however, are getting bypassed in modern healthcare. With the systematic tendency to measure service in terms of time and time in terms of money, today’s electronic health care record systems force stories into checklists. Listening to stories is harder than filling out checklists. While these tendencies chip away at our ancient profession we can fight the trend. When we make a choice to listen, as Hugh advocates, clinical medicine becomes an art.
Seven. Art & medicine. In 1936 Sir Henry Wellcome’s will established the Wellcome Trust in London to advance medical research and the understanding of its history. If you visit that city the Wellcome Trust is a wonderful place to spend a morning or afternoon perusing its collections and exhibits. An article last year in JAMA by Jeremy Farrar, Director of the Wellcome Trust, discussed the role of this organization in the world today. [Farrar. Science, medicine, and society. A view from the Wellcome Trust. JAMA. 313:2315, 2015] The trust expends more than $1 billion dollars yearly in biomedical sciences and biotechnology “interrogating the fundamental processes of life in health and in sickness and using that knowledge to develop ways to promote well-being and to diagnose, treat, or prevent disease.”
Farrar makes the point that while science is essential and wonderful, its implementation in medicine and society is not guaranteed. He references Semmelweis and Snow, who in the mid-nineteenth century provided theory and supporting evidence that certain diseases were transmitted by dirty hands, yet conventional wisdom of the time rejected the idea. Farrar writes: “…their stories reveal that scientific evidence is not enough to improve medicine: social and cultural factors are vital as well… Because the Trust appreciates the importance of the history and social contexts of medicine, it also supports research across the medical humanities, social sciences, and bioethics, as well as funding for artists and educators to engage the public with research.”
We health care professionals revel in science. Scientific ways of thinking have brought us a verifiable understanding of life, health, and illness as well as new technologies to enhance health and mitigate disease. Yet as Farrar tells it, science is not enough. History, social contexts, and values must always frame the science, as well as inspire and deploy it. In the consilience of human knowledge, as EO Wilson explains, science is but one facet of the art of Homo sapiens.
Eight. Chang Lecture on Art & Medicine. In 2007 our Department of Urology began an annual lecture in honor of the family of Dr. Cheng-Yang Chang, an esteemed Nesbit Alumnus who joined our faculty when Urology was a small section of the Surgery Department. Dr. Chang was our first faculty member to focus on pediatric urology. Coincidentally, his father was a highly acclaimed artist in China during its turbulent mid-Twentieth Century years. A number of his paintings are housed in the University of Michigan Art Museum where you can also visit the Shirley Chang Wing, named in honor of Dr. Chang’s late wife. The couple had two sons. Ted Chang, a University of Michigan and Nesbit alumnus like his dad, practices urology in Albany New York. Ted is a first class urologist and educator. Hamilton Chang, a fellow UM man, is an investment banker in Chicago, a leader in Michigan’s alumni organizations and a cornerstone of our urology fundraising efforts.
This year’s Chang Lecture will be given by Don Nakayama, a pediatric surgeon and expert on the Diego Rivera Murals you can find at the Detroit Institute of Art. The Surgery Panel on the upper left hand corner of the south wall has been described by art historians as “brain surgery,” but after personal investigation Don discovered that the art historians were not quite right, anatomically. The actual panel, in fact, depicts an orchiectomy, an operative procedure far more in tune with Rivera’s theme, as a committed socialist, of the emasculated worker. Don discussed this in a paper in The Pharos, [Summer 2014, p. 8].

[Above: south wall. Below: surgery panel]

If you plan to visit the Ann Arbor Art Fairs this July, consider setting aside an hour to join us at the Chang Lecture on Tuesday, July 21 at 5 PM in the UM Hospital Ford Auditorium. You can hear Dr. Nakayama, meet him at a reception after the talk, collect some CME credits if you are a physician, and have your parking ticket stamped. Not a bad deal, I submit.
Nine. The art of humanity extends from the earliest moments of assisting childbirth, caring for lacerations, splinting fractures, counseling sufferers, and painting on cave walls, to today’s robotic surgery and technological entertainments such as the new Star Wars, if you accept the proposition that art is any deliberative human action or construct. This new iteration of Star Wars successfully expands the story of a distant galaxy and the force that binds it. A business school professor at Washington University St. Louis explored the narrative and proposed that an economic force binds the distant galaxy as well, thus brightening the dismal science. [http://arxiv.org/format/1511.09054v1]
The dark side of the dismal science was evident in another current film – The Big Short. I’d read the book by Michael Lewis, who showed in lucid detail how the housing and credit bubble collapse in 2008, known also as the subprime mortgage crisis, was predicted. This catastrophe quickly expanded into a major stall of the world economy, that is still under repair. The astonishing thing is that the prediction was not made by economists, the big banks, the big accounting firms, universities, Nobel Laureates, bond rating companies, regulatory agencies, or “the market” itself. The prediction was made by an oddball physician who analyzed publicly available data and discovered the “obvious” flaw in complex mortgage securities. Astonishingly, none of the experts was so smart and the sad, sad reality is that none of them was doing their job competently. This story begs the question: how can so many smart people be so dumb? It’s an astonishing story and a very cautionary tale of reliance on experts. If course we have to trust experts, but we also have to verify that trust constantly in real time, by listening to diverse and even oddball opinions and insisting upon honest broker regulation and competition.
The physician who figured this out was Michael Burry, a UCLA economics graduate, Vanderbilt MD, and Stanford neurology resident. His main interest, however, was investing and even as a resident had acquired a reputation for success in value investing. He left residency to invest full-time and in November 2000 he started Scion Capital. As Lewis told the story, in the first full year of Scion when the S&P 500 fell 11. 88%, Scion’s fund was up 55%. This was no Bernie Madoff effect, the Scion success was real, verifiable, and durable. Value investing is based on the idea of buying an asset that appears underpriced according to an analysis of some sort. The analysis may recognize some fundamental flaw in the current price of the asset based on historical factors, operational data related to the company, information about its market and competitors, or expectations concerning the future. In some ways this is a complex extension of the thinking of Martín de Azpilcueta. Burry extended the idea by betting against the future value of money through an insurance mechanism called the credit default swap.
Burry was not looking for “a short” rather was actually seeking good long term bets. In 2005, however, his analysis of national lending practices in 2003 and 2004 indicated to him that a subprime mortgage bubble would collapse in 2007. He persuaded Goldman Sachs to sell him credit default swaps against certain subprime deals. The rest is history, as well as excellent cinematography.
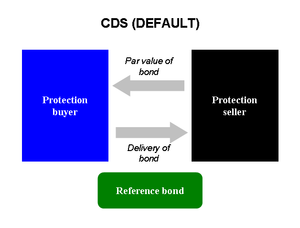
[Illustration: Lamro, on Wikipedia, Credit Default Swap. Burry is the blue box, Goldman Sachs is the black box. The par value of the asset was its high value at the time of the credit default deal.]
Ten. March, now that we are a few days into it, has its own stories. March 1 is the meteorological beginning of spring, although that may not be so apparent here in Ann Arbor. March 20/21 is the astronomical beginning of spring in the Northern Hemisphere or autumn in the Southern. The month is named for the Roman God of War, Mars, who was also the guardian of agriculture. This was an odd conjunction since it is not immediately apparent that the pursuits of war and of agriculture are similar. On the other hand, if you believe that the best defense is a strong offense, the idea makes some sense and in Roman times the month Martius marked a new season of farming and military campaigns. In addition to competence on the land and in battle, legend also ascribed to Mars some competence in the urological sense, as his relationship with the Vestal Virgin, Rhea Silvia, produced twin boys, Romulus and Remus, the mythical founders of the city of Rome. Even beyond the reproductive outcome, Mars was generally viewed as a paragon of virility, with no issues of low testosterone. Martius was the start of the Roman yearly calendar until as late as 153 BC. Russia held on to this start date to the end of the 15th century, and Great Britain and its colonies (even us in America) used March 25 as the beginning of the calendar year until 1752 when the Gregorian calendar was adopted. March is American Red Cross Month.
March 13 marks the shift to Daylight Savings Time. Ben Franklin has been claimed as originator of daylight savings time, but in fact the solid proposal came from George Vernon Hudson who died 70 years ago (5 April 1946). Born in London he moved to New Zealand with his father and became a respected amateur entomologist and astronomer. His daytime job in Wellington as post office clerk gave him time after work to study and collect insects. It was said that this was the impetus for his idea to maximize daylight in winter times. In 1895 he gave a paper at the Wellington Philosophical Society proposing a 2-hour daylight savings time shift. Hudson was a member of the 1907 Sub-Antarctic Islands Scientific Expedition. The daylight savings idea was slow to catch on and New Zealand’s Summertime Act wasn’t passed until 1927.

[Left: Hudson in 1907 on expedition. National Library of New Zealand. Right: Willett in 1909, J. Benjamin Stone Collection, Birmingham Central Library.]
Daylight savings occurred later to another Briton, home builder William Willett (1856-1915). Riding his horse one summer morning he observed many household’s blinds still drawn, indicating the inhabitants were still asleep and missing much of the day. He began to advocate for an official way to extend daylight and the British Summer Time became law in 1916, although Willett died just before it went into effect. (Trivia: Willett’s great-great-grandson is Chris Martin of the band Coldplay.) Today, daylight savings time methods are utilized throughout much of the world.

[Wikipedia. Blue – DST used, Orange – formerly used, Red – never used]
If March came in like a lion we hope it exits sheepishly after a bit of collegiate athletic madness. We also will be having a departmental retreat at the end of the month. Before closing out this message, let me return briefly to Ben Franklin, printer, inventor, author, postmaster, diplomat, and urethral catheter expert. In 1752 he designed a flexible silver catheter for his brother John who was suffering from bladder calculi and it is likely that, living to age 84, Ben used it himself.
Thanks for reading What’s New and Matula Thoughts.
David A. Bloom, University of Michigan, Department of Urology
