
Matula Thoughts August 1, 2014: Art & medicine
This is the blog format of the monthly email communication called “What’s New” from the University of Michigan Urology Department.
1. 
My drive home from work in the summer is likely to occur in cheerful sunlight, even when the hour is late. A good piece of this seasonal pleasure still remains for us at the start of August. July 2014 has come to a close and with it the celebration of the Fourth, the Ann Arbor Art Fairs, and the Chang-Duckett-Lapides Lectureships of the Urology Department. Our PGY1s (interns) class of 2019 began at least five years of residency training that may easily extend by several additional years with fellowships that many of our graduates undertake. The lectureships we hold every year around this time add some formality and socialization as the new academic season of residency training commences. Andrew Kirsch of Emory University gave a remarkable Duckett Lecture on his work with magnetic resonance urography (MRU) and Kassa Darge of the Children’s Hospital of Philadelphia produced a superb Lapides Lecture on the wide scope of urologic imaging and his experience with MRU. We had excellent attendance and wonderful discussion. MRU is clearly the new IVP. Yes, it is at present much more costly, but as we saw in the discussions, a careful history and physical exam with high quality GU ultrasonography in the hands of well-trained and experienced clinicians will answer anatomic questions well enough to deal for most problems we see. In complex situations, however, the detailed anatomic and functional information from the MRU is unsurpassed. George Drach of the University of Pennsylvania presented a clear discussion of a muddy topic – the Affordable Care Act. He promised that the topic will get even muddier next year as complex add-on legislation accrues in the year ahead.

[Andrew Kirsch, Duckett Lecturer, with Susan Kirsch]

[Peggy Duckett, George Drach, & Kassa Darge, Lapides Lecturer]
2. The Chang Lecture on Art and Medicine (our 8th) was given by James Ravin, a well-known ophthalmologist from Toledo who had trained here in Ann Arbor. I first learned about him through his book, The Artist’s Eyes, which had been sent to me by Steven and Faith Brown, Michigan alumni and strong supporters of Michigan Urology. The lecture was amazing and we can mail you a CD of the lecture if you send us a note. Before Dr. Ravin took the microphone, I asked the audience: Why should a urology department care about the link between art and medicine? My answer was twofold and I’d like to repeat it here. The first reason is simply the matula. This long-standing symbol of the medical profession is the flask used for the macroscopic examination of urine. Not insignificantly that is also the name we selected for this blog. The second reason is that this linkage is hardwired in our species. Genetics and epigenetics demand this attention from us. Maybe this is a presumptive conceit, but most people believe our existence among life forms is unique and that the distinctive human condition we claim is built upon our curiosity, our creativity, and our tendency to reflect upon ourselves as well as our fellows. These traits have led to our ability to solve problems cooperatively and accomplish complex tasks like building cathedrals, performing symphonies, writing encyclopedias, or doing cystectomies and urinary diversions. Art is part of all human performances, most especially the medical arts.

[Hamilton Chang, James Ravin – Chang Lecturer, & Dr. Cheng-Yang Chang]
3. That the study of art should occur in a university is no surprise, universities are the primary stewards of the future – the human future and the global future. Universities educate tomorrow’s builders, thinkers, and citizens. They and their graduates are the primary sources of tomorrow’s ideas and inventions. No other institution in society has such a broad mandate, much less fulfilled it so well over centuries as universities. Ben Shahn, an American Artist of the second part of the 20th century, put together an essay in a book called The Shape of Content in 1960, where he specifically addressed the matter of visual art in universities, writing: “What can any artist bring to the general knowledge or theoretical view of art that has not already been fully expounded? What can he say in words that he could not far more skillfully present in pictorial form? Is not the painting rather than the printed page his testament? Will he not only expend his energies without in any way increasing the general enlightenment? And then, what can an audience gain from listening to an artist that it could not apprehend far more readily simply by looking at his pictures?” While Shahn was specific that his comments related to visual art, his point extends more broadly.
4. Shahn answers his own questions in the essay, developed from lectures at Harvard College and offers two reasons why universities (and by extension medical schools and their departments) should be interested in art. First, the product of universities, educated persons, should have what he called the accomplishment of perceptivity – a necessity for tomorrow’s international citizens. His second reason is that the universities, themselves, are enriched by bringing art, he says, into the circle of humanistic studies. This point anticipates the vision that E.O. Wilson called consilience, the idea of global village of knowledge in which boundaries between fields of study are mere human conceits. Wilson contends that the most important findings for our species will be made at the interfaces and boundary waters among the fields. Shahn expands on this second point in his essay, saying that bringing art into the circle of humanistic studies serves the: “… general objective of unifying the different branches of study toward some kind of a whole culture. I think it is highly desirable that such diverse fields as, let us say, physics or mathematics, come within the purview of the painter, who may amazingly enough find in them impressive visual elements or principles. I think it is equally desirable the physicist or mathematician come to accept into his hierarchy of calculable things, … [the] nonmeasurable and extremely random human element which we commonly associate with poetry or art.” [Shahn p. 9]
5. Visiting professorships are an important part of academia, bringing the best insights of established thought leaders, as well as the newer voices and controversial ideas of those who challenge the status quo. We do this fairly well at Michigan Urology throughout the year in each of the disciplines within our field. It is equally and especially important for universities to offer periodic public lectures on broad themes such as Ben Shahn provided at Harvard for general audiences on topics that offer important humanistic insights, cut across fields of study, and stimulate conversation and cultural curiosity. We try to fulfill our part with the Chang Lecture and if you missed it this year, consider holding that calendar slot next year on the Thursday of the Art Fairs. Our speaker will be Pierre Mouriquand of Lyon, France. He is an extraordinary pediatric urologist, a deep thinker, and a committed artist who paints nearly every day.
6. A number of years ago I came across a wonderful statement made by the late and great Michigan faculty member and world-class physiologist, Horace Davenport. A student recalled him telling a medical class that “physicians are the attendants at the service station of life.” Of course, in Dr. Davenport’s days the gas stations were true service stations where someone pumped your gasoline, checked your oil and tires, washed your windows, and actually fixed problems with your automobile. Notwithstanding the dated image of the service station, it is an appealing metaphor. While the current phrase patient-centered care is bandied about as though it were a new idea, the consideration of “what the patient wants” has really never been far from the minds of good physicians. While we all have seen instances of domineering and inconsiderate medical care, the idea of a “patient-centric” approach is hardly revolutionary and new. It is unfortunate, albeit useful, that we need to proclaim that the health care we offer in our organizations is “patient-centric.” As health care has become more complex, specialized, and team-based it is easy to retreat onto islands of our professional turfs and focus on the solutions of isolated clinical problems. This professional convenience, however, turns patients and their inevitable co-morbidities of modern life into mere packages of DRGs in search of CPTs. The complex billing systems we dignify with the phrase modern electronic medical records are more than innocent co-conspirators in this crime. The success of the modern health care enterprise will depend on its ability to simultaneously fulfill the desires and needs of each patient in the contexts of their physical, emotional, and social problems. This will require teams and systems that are at once lean and adaptive.
7. Long before science impacted the work of physicians, medicine was described as an art and I believe there still is much art to our work insofar as you might look at art as anything that is choice. Science and evidence cannot and will never define all of our choices in medicine. Two fundamental questions define modern health care. The first is: what does the patient (and family) really need and want? The second is: what does society want from its health care enterprise? The answers to the two questions are quite different. It is the first question that drives our essential transactions in health care, patient-by-patient and family-by-family. Of course these transactions must exist in the framework of society and the sense of what is right and reasonable to do for each individual patient. On the other hand as we create public policies and deploy health care systems, the second question comes heavily into play and begs the question: how much should a nation spend on the well-being of its people? So is 20% of GDP, for example, too much or is it not enough? It’s interesting to compare health care to food expenses. In some nations, families spend 60% of their household income on food, while in the USA food accounts for less than 10%. Granted that individual household expenses and national GDP are very different “apples and oranges” and the constraints of a nation differ from those of a household, it is clear that the more one expense dominates a budget the less remains for other necessary and desirable expenses. As a matter of public policy, however, ideally how much should a nation spend on its health care? How much on the education of its next generation? How much on its self-defense, on its research & development, on its infrastructure depreciation, or on its service of past debt? However you answer these questions, it is a fact that in the USA we are moving towards 20% of GDP for health care, and other advanced nations are not terribly far behind and moving towards us. That being said – a good third of the expense is generally recognized as waste – money spent that helps neither patients nor society.

[Table from The Economist]
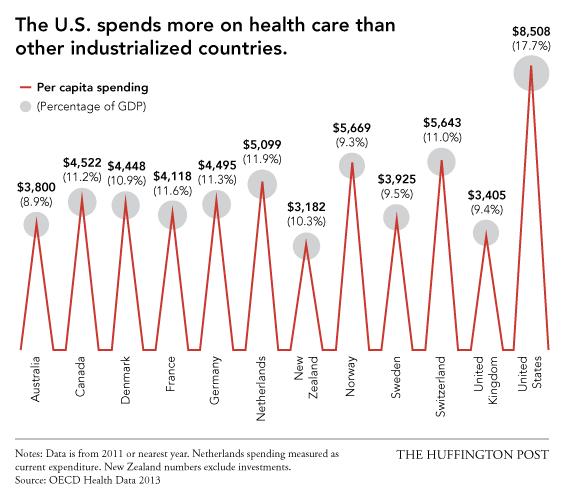
[Huffington Post July 10, 2014]
8. An interesting point of view, written 2 years ago in the New England Journal of Medicine by MJ Barry and S Edgman-Levitan, called Shared Decision Making discussed a Picker Institute report that identified eight characteristics of care as the most important indicators of quality and safety from the perspective of patients. These characteristics are: respect for patient values, preferences & expressed needs, coordinated & integrated care, clear information & education of high value for the patient & family, physical comfort with alleviation of fear & anxiety, appropriate involvement of family & friends, continuity, and access to care. This list mirrors a more simple set of things that I believe patients want, since these are the simple things I want from my personal physicians: kindness, expertise, and convenience. Perhaps the attributes you might list would differ in number or terminology, but I think most people want roughly the same things. [MJ Barry and S Edgman-Levitan, Shared Decision Making. NEJM 366:780, 2012]
9. 
I’ve shown this picture before in our Department of Urology “What’s New” column, but am compelled to share it again. The picture appeared on the cover of JAMA, a fact that dates this work since for the past year or so the new editor of the journal, Howard Bauchner, while he retained the art feature, moved it from its long-standing place on the cover of each issue. [JAMA 3017:2497, 2012. Toll E. The cost of technology. Copyright 2011 Thomas Murphy] Change is inexorable, however, and I have to say that he has done a superb job with the journal, both in format and in topic selection. The illustration shown (with previous permission of the author, Elizabeth Toll) shows a crayon drawing of a scene in a doctor’s office. The 7-year old artist drew her sister sitting on the examining table looking at the viewer in a most Vermeer-like fashion. Mother, with a younger child on her lap, is seated at the far right. The artist sits in between, at work on her picture, but also gazing intently at the viewer. The astonishing feature of the artwork however is the physician sitting at the far left, totally absorbed at the keyboard in the technology that is mandated in healthcare. The software has become a surrogate for the patient. The artist told it as it was and, no doubt the physician felt some shame on viewing the artwork. The enormous sums of money we have been forced to expend on clunky and dated software, compliance for poorly fashioned regulation, and the turmoil of the restructuring of a massive industry are a significant part of the waste. What will the next generation of health care look like when we leave behind the RVU, meaningful use, EPIC, and ICD-10? Such a world cannot be too far away. We hope academia, industry, and public policy can put together systems that are accessible, fair, lean, adaptive, and good for patients.

[Jeff Halter, Howard Bauchner, Preeti Malani, & Eve Kerr at a reception at Preeti’s home 2013]
10. The well patient exam has been challenged as “unnecessary.” So too has the routine pelvic exam, the PSA testing, and even routine urinalysis. This brings me to the question, what is the point of healthcare? As physicians we like to solve and fix problems of patients, but is that all that patients really want? Yes, often a patient comes with a very specific problem, but very often not all the problems are evident and sometimes they are deeply entangled with the other issues we like to call co-morbidities. This brings me back to Dr. Davenport’s thought. People and their cars have to stop at service stations from time to time. Sometimes they need gas or have a flat tire. At times the car isn’t working well and help is needed of one sort or another, but the problem isn’t immediately evident and the attendant must diagnose before repair. It is also useful, at other times, to have an expert look at the car, see how it runs, listen to the engine, and check under the hood. Preventive maintenance and inspections may discover occult issues for which early intervention can prevent serious harm. I can’t believe this isn’t true for human bodies and minds. People need to stop by the service stations of life from time to time just as well, for after all we are susceptible to far more ills than our motor vehicles. A doctor, or other health care provider, can look, listen, counsel, advise, and teach. The pastoral side of a doctor’s art should still be a major part of the toolkit. Not every problem discovered needs remedy, but every person should be seen, listened to, and examined periodically by some kind and expert attendant at the service stations of life where art and medicine converge. This is how we care for the human condition.

[1936 Union Gas Station. Main & Weatherlow. Lassen County History. Wikipedia – Historic gas stations]
Best wishes, and thanks for spending time on “Matula Thoughts.”
David A. Bloom, Department of Urology, University of Michigan
