Matula Thoughts March 5, 2021
2987 words
Politics, as usual?
One.
Last month was Lincoln’s birthday and a new biography, Abe by David Reynolds, merits comment. Fundamental issues of Lincoln’s times remain fundamental issues today and Reynold’s book permits you to be a “fly on the wall” in the rooms where consequential things happened. You need not be historian, constitutional lawyer, or elected politician to weigh in on these issues – literacy in today’s complex world is an existential necessity, political literacy for health care professionals in particular.
Lincoln took office at an extraordinary moment of bitter partisanship and threat to the nation. His first inauguration was preceded by ugly political fighting amidst divisive and turbulent social conditions that Lincoln navigated deftly, although sometimes uncertainly. Many ideologies, “isms” and factions created a toxic climate that divided the nation into uncompromising strongholds of opinions as to which way the country should go. Lincoln was the consensus choice of the voters, but his perceived ideology was contentious to a vocal minority.
A recent article by historian Ted Widmer tells how on February 13, 1860 (a day after Lincoln’s 51st birthday) a mob tried to enter the Capital to disrupt the confirmation of the election. The mob, lacking passes to enter the Capital (and ignoring how American democracy was intended to work with peaceful transfer of presidency), was blocked by soldiers and protested loudly outside the building. Tempers also flared inside House and Senate chambers but American democracy and Lincoln won that day at the Capital. [T. Widmer, NYT, Jan 10, 2021.]
Reynolds argues convincingly that Lincoln distilled the toxic climate of opinions and centered his political course on the central defining idea of the nation as he saw it,
“.. Slavery, he declared in August 1856, ‘should be not only the greatest question, but very nearly the sole question.’ Noting the diversionary tactics of the proslavery side, he stated, ‘Our opponents, however, prefer that this should not be the case.’ He again drove home his main point: ‘The question is simply this – should slavery be spread into the new territories or not? This is the naked question.
Along with the naked question went a central idea. ‘Our government rests in public opinion … Public opinion, on any subject, always has a central idea, from which all its minor thoughts radiate. That central idea in our political public opinion, at the beginning was, and until recently has continued to be, the equality of men.” [D. S. Reynolds, Abe, Penguin Press, 2020, p. 434-435.]
This was a historically sound and prescient argument. Lincoln boiled down the entire national acrimony to the single organizing (and aspirational) principle of the Declaration of Independence – human equality.
Inasmuch as the Declaration was the primary justification for the new nation, it was an obvious corollary for Lincoln that the nation could not be divided, leading him to the famous biblical reference in his House Divided speech of June 1858.
“ ‘A house divided against itself cannot stand.’
I believe this government cannot endure, permanently half slave and half free.
I do not expect the Union to be dissolved – I do not believe the house to fall – but I do believe it will cease to be divided. It will become all one thing, or all another.” D.H. Donald, Lincoln. Simon & Shuster, NY 1995. p.206.]
For all the subsequent debate over the conflict between the aspirations of the Founders and the ugly facts of “state’s rights” to hold human beings as “property,” the reality is that neither the Declaration nor the Constitution provided for such personal rights to own property in human beings – a concept totally dissonant from the foundational mandate and words of the Declaration.
Both documents had required consensus among all 13 colonies. Three provisions of the Constitution reflected the wills of slave-holding states, yet the document deftly steered clear of asserting any claim to the noxious idea of human slavery itself – “property in man.”
The first Constitutional provision (Article I, Section 2) allowed for congressional representation and apportionment of taxes for the states based on their “respective Numbers” of “free Persons” (these were assumed to be white men only, although that was never explicitly stated) plus:
“…those bound to Service for a Term of Years, and excluding Indians not taxed, three fifths of all other Persons.”
This cynical inclusion gave the slaveholding states the extra edge of additional votes and tax reapportionment for three-fifths of all enslaved persons. Ultimately these provisions were obliterated by the Thirteenth and Fourteen Amendments.
The second provision, another bone thrown to the slaveholding states, came in Article 1, Section 9 but it was time-limited.
“The migration of Importation of such Persons as any of the States now existing shall think proper to admit, shall not be prohibited by the Congress prior to the Year one thousand eight hundred and eight, but a tax or duty may be imposed on such Importation, not exceeding ten dollars for each Person.”
The final provision is in Article IV Section 2:
“No person held to service or labor in one state, under the laws thereof, escaping into another, shall, in consequence of any law or regulation therein, be discharged from such service or labor, but shall be delivered up on claim of the party to whom such service or labor may be due.”
The framers of the Constitution clearly expected “property in man” to wither away, little expecting the Missouri Compromise of 1820 would allow the inclusion of a new slaveholding state and the Kansas-Nebraska Act of 1854 would allow the “popular sovereignty” of new states to make their own decisions on the matter. Rather than withering away slaveholding was resurgent in the days leading up to Lincoln’s first term and civil war was inevitable.
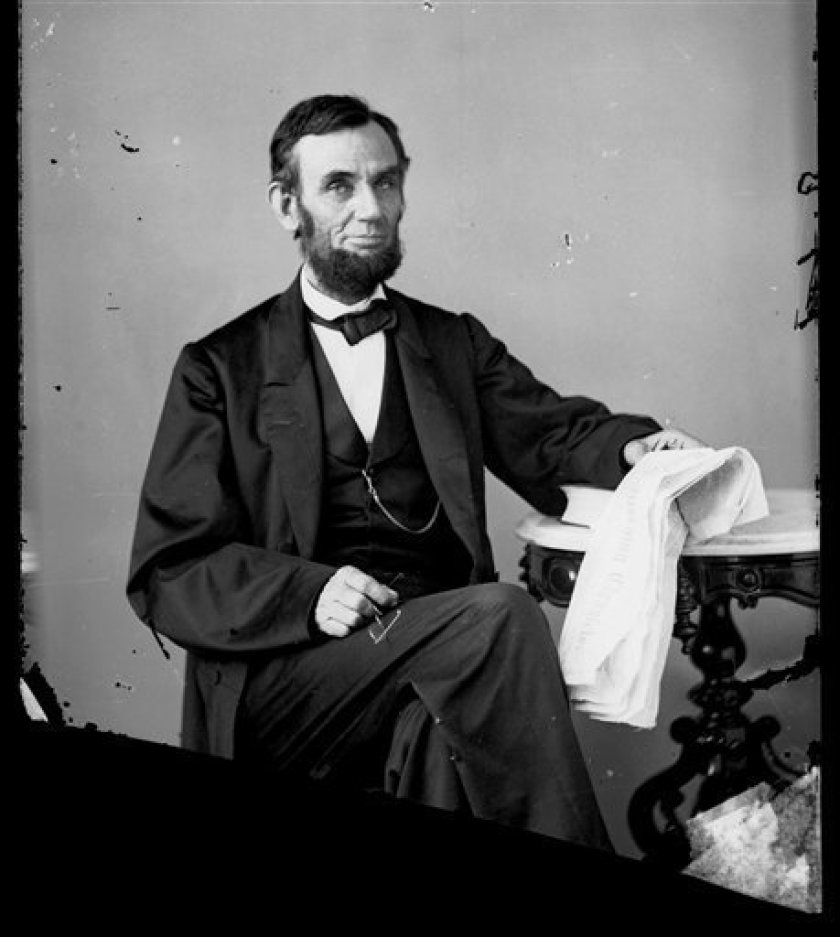
Lincoln set a course for the war with principle and perseverance, although as it ground on undecidedly, the Union will flagged and Lincoln feared for his reelection. By July 1863 the tide turned, in spite of draft riots in NYC, and Union victories in Vicksburg and Gettysburg fueled optimism. In August the president decided to sit for a picture.
Photographs in those days required long exposures, lasting many seconds or minutes and, as Lincoln sat for a glass plate portrait in August 1863 at Alexander Gardner’s studio in Washington, a fly alighted on the president’s trouser leg below his right knee. Lincoln was unperturbed and continued to sit still for the photograph, without troubling the insect. [Above: Gardner’s photo. Below: detail of the famous fly under Lincoln’s knee on the posterior crease.]

Two.
Health care in Lincoln’s time hardly compares to health care today, but the matters of human inequality in terms of life, liberty, and the pursuit of happiness underpin our modern acrimony just as they underpinned the great national dilemma in 1860, especially so today in matters of health care. [Above: Harper Hospital, original hospital complex in an 1884 drawing 710 of The history of Detroit and Michigan or, the metropolis illustrated …, by Silas Farmer p. 710. British Library.]
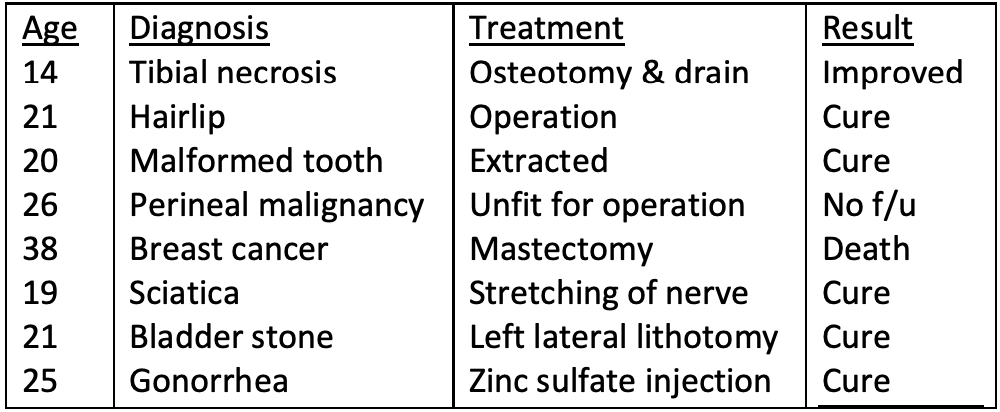
In Lincoln’s lifetime it was unusual for a person anywhere in the world to go into a hospital. Medical care was delivered in doctor’s offices, people’s homes, or on battlefields. Hospitals offered very little to their unfortunate patients, aside from a bed. Lincoln died just when the germ theory emerged from Ignaz Semmelweis, Louis Pasteur, and Joseph Lister. The medical world was starting to change. During the Lincoln presidency, Ann Arbor had no hospitals, while Detroit had several, the newest being Harper Hospital, built in 1863, largely to attend to soldiers injured during the Civil War.
Health care reflects the values and aspirations of economic and political systems of any given community and society. Modern nations seem to be see-sawing between democratic rule and authoritarian/central rule. Yet this is not a simple bipolar contest. Democratic rule provides elected representatives to express “the will of the people” but requires significant central/federal authority that may verge toward authoritarian leadership (as was claimed during FDR’s presidency on numerous occasions). Authoritarian control of a society responds poorly to the needs of the people, stifling education, inquiry, and innovation but is ultimately (and ironically) contingent on acceptance of that authority by enough people in the society (as revolutions have proven again and again). As Lincoln said, our government rests on public opinion. And public opinion should be informed by basic Constitutional literacy.
A scathing critique of modern hospital care is recounted in the recent small book by noted historian Timothy Snyder, Our Malady. Lessons in Liberty from a Hospital Diary. He offers the provocative opinion that liberty in the political sense and health care in personal terms are directly linked, gleaning that perspective from his near-fatal illnesses and suboptimal hospital care.
“America is supposed to be about freedom, but illness and fear render us less free. To be free is to become ourselves, to move through the world following our values and desires. Freedom is impossible when we are too ill to conceive of happiness and too weak to pursue it. The word freedom is hypocritical when spoken by the people who create the conditions that leave us sick and powerless. If our federal government and our commercial medicine make us unhealthy, they are making us unfree.”
Three.
Freedom of enterprise and thought have brought great accomplishments in medicine and science but not a unified system of heath care. We often are told “Our health care system is broken” but the complaint is not quite right. No purposeful system exists, rather a variety of organizations and systems that have evolved in response to the myriad needs and challenges of healthcare. Each system may work well enough for its purposes and stakeholders, but they function independently, often in competition with other systems and their stakeholders. The common good of the public, individually and at-large, tends to be a secondary concern. The “broken system” complaint, although misconstrued, is relevant and global. The individual patient is the ultimate stakeholder, but gets lost in the systems.
Health care should be many things – accessible, equitable, effective, efficient, timely, safe, kind, and universal. But it usually falls short. This is obvious to 7 billion people – advantaged and disadvantaged populations alike. Local, regional, and global inequities are visible every day on public streets or in countless newsfeeds. Even if your individual health care seems secure, it is precarious – predicated on a job, a bank account, health status, social status or caste, location, family member, public safety, and other particularities.
The frameworks of healthcare organizations reflect the values that underpin them in each locality and their nations. Most perform adequately in terms of their business success, some excellently, but few do well in the matters of personal care, coordination, excellence, equity, and value. Business success (revenue optimization) is not the primary purpose of non-profit healthcare organizations. That’s not why society grants them no-for-profit status.
The State of California recently sued Sutter Health for anticompetitive practices that raised the cost of health care in northern California for little reason beyond increase in revenue.
We, the public, should care about this. Most large health care organizations enjoy the benefit of “non profit” status. The public gives these organizations tax breaks that are not given to “for profit” organizations like Amazon, Exxon, or Johnson and Johnson, that have a central defining objective of maximizing shareholder value. “For profit” organizations of course have other protections carved out by the public, notably limited liability status, that enhance their abilities to succeed in the business world, but “not-for-profits” serve larger public values.
Four.

Management by accounting uses performance metrics and these have spread into the non-profit sector, health care in particular. Metric domination tends to deform missions. When governing boards use performance incentives to inspire a CEO, CFO, or CMO to cut nursing positions, eliminate overtime, or decrease benefits, then those things are likely to happen even if they damage the quality of products, the performance of employees down the ladder, or the culture of organizations. The entire brand of any organization is at risk, not-for-profits especially. Governing boards optimally should govern and not manage (and micromanage) their organizations. They need wise management leaders with holistic (and accountable) reign over their domains in the organization to best advance the mission of the enterprise, which naturally involves financial responsibility but not to the detriment of mission or brand. [Above: bean counting. Illustration from Margarita philosophica, 1503, by Gregor Reisch (d. 1525). Houghton Library, Harvard University.]
Financial responsibility in health care, essential as it is, cannot not be constrained to the next quarter’s balance between revenue and expenses. Immediate “financial margin” is important, but no less essential are quality, value, stakeholder satisfaction, financial liquidity, investment in enterprise strategy, investment in research and innovation, health care education, debt leverage, leadership succession, community responsibility, workforce health-retention-recruitment, organizational culture, policy development, public health, etc.
Health care is a huge and complex bucket of obligation in the modern world, far too complex for any of its myriad organizations to be primarily managed by key performance indicators or incentive directives.
Five.

Presidential inaugurations used to occur at this time of year because slow communications and clumsy political processes of this nation in its earlier history required at least four months from national elections to the peaceful transition of power that distinguished the American experiment in democracy.
The first inauguration, that of George Washington, took place on April 30, 1789, but subsequent ones occurred in March until March 4, 1933, the last March presidential inauguration, when Franklin Roosevelt replaced Herbert Hoover (above) – after a contentious election in the dark days of the Great Depression, but the two statesmen executed a graceful transfer of power in the finest tradition of American Democracy.
New technologies of communication and shortened news cycle in Roosevelt terms allowed inaugurations to be moved to January – the second inauguration of Roosevelt was the first of these after the Twentieth Amendment to the U.S. Constitution moved the beginning and ending of presidential, vice presidential, and congressional terms from March 4 to January 20.
The past presidential election degenerated into fraudulent claims of voting irregularity, dozens of dismissed lawsuits to overturn results, and efforts to block the transition of power by congressional mischief or threat of armed force. The election results were counted, recounted, inspected, certified, and ligated over two months, but cynics may seek to restore that original prolonged interval between actual election and inauguration to allow more time for shenanigans.
Unfortunately, something so important as political leadership falls into the hands of all sorts of men and women called politicians, whom history proves again and again cannot be uniformly trusted to “do the right thing.”
This ultimately comes down to personal assessment, but what are the right things? Are they the right things for politicians, their constituencies, or the right things for society at large? The answers comes back to the Declaration and Constitution: life, liberty, and pursuit of happiness with Constitutional fidelity. This means fair and equitable education, justice, public health and safety, and opportunity. Much of this is measurable with public health and safety data, poverty statistics, crime rates, equity in housing and education, and “happiness” ratings such as Likert score surveys.
Roosevelt’s four terms derived from democratic elections and he functioned with a strong hand, discovering new essential federal roles in rebuilding a nation from economic collapse and then guiding it successfully (along with much of the rest of the world’s nations) through a massive war. Hitler, in contrast, manipulated his appointed position as chancellor into authoritarian rule that precipitated and lost that war, incurring unimaginable devastation in his 12 years as dictator.
Political systems, transcending individual leaders and terms, are essential to carry out the “will of the people” and protect them from threats whether they be human threats, economic threats, biologic threats, or environmental threats. Political literacy is an existential necessity.
Postscript.

On the walls.
Metaphoric elevation of lowly and annoying houseflies (Musca domestica) to miniature sentient journalists imagines the precarious nature of the invertebrate, in imminent danger of destruction by authoritarian swat. [Above: Housefly, Wikipedia.]
A related metaphor, the bugging of a room, came to life in the real world and literary genres of crime and spy stories.
After President Obama successfully eliminated an annoying fly during a CNBC interview in June 2009 a number of journalists recalled Lincoln’s greater tolerance in August 1863. The organization People for the Ethical Treatment of Animals (PETA) chastised Obama mildly and sent him a “handy-dandy bug catcher” according to its newsletter Animals Are Not Ours. [Alisa Mullins, “Obama and the fly,” June 17, 2009.]
This was not President Obama’s last public brush with the unruly insect order, it happened again in January 2013 during a White House briefing when he announced his selections to head the Securities and Exchange Commission and the Consumer Financial Protection Bureau. An emboldened fly briefly alighted on Obama’s forehead, but escaped to buzz another day, although journalists were quick to record the event. Vice President Pence, among countless others, also had his historic moment with Musca domestica, at the October 2020 Vice Presidential debate, once again showing that politicians sometimes tolerate flies on the walls and bugs in the rooms where things happen.
American re-enlightenment. The George Floyd moment of 2020 illuminated much of the American condition from its original sins to present disparities that so impact the aspirations of life, liberty, and the pursuit of happiness.
My friend and Army colleague, pediatric surgeon Victor Garcia, recently sent me a book by a teacher at his alma mater, West Point, Ty Seidule. Robert E. Lee and Me. A Southerner’s Reckoning with the Myth of the Lost Cause. This timely book, explains how attitudes are formed in cultures, how they persist, and how or why they can change. [T. Seidule, St, Martin’s Press, NY. 2021.]
The difficulty of changing beliefs and myths – through rational argument, historical analysis, and scientific process – is an existential challenge that our species seems to be failing. Flies on the walls watch and invertebrates may yet win the day on this planet, even though Homo sapiens is capable of doing so much better.
Thanks for looking at Matula Thoughts, March 5, 2021.
David A. Bloom
University of Michigan, Department of Urology