WN/MT October 2, 2020
Quilting bees and blues
2392 words
One.

October Blues. Historically at this time of year, the blues came from regret over the loss of summer and the expected hunkering-down for winter ahead in the northern hemisphere. October 2020, however, finds most of the world already hunkered down for Covid-19. Students had another cause for October Blues, after the emotional rush of new school terms in September gave way to the “boring” routines of schoolwork, boredom that is now a matter of fond nostalgia.
No one can reasonably deny that schooling is essential to pass along skills and knowledge to successive generations. The processes and environments of schooling, in all its forms, also provide opportunities to improve the actual knowledge and skills, as well as forge community values. The present pandemic reaffirms that schools are a cornerstone of society at K-12 levels for socialization of students and for liberation of parents to do their daytime work. Higher education and the myriad forms of schooling beyond traditional schools are no less essential, but sharply compromised by pandemics that, recurring as we know well, should not take us so completely by surprise.
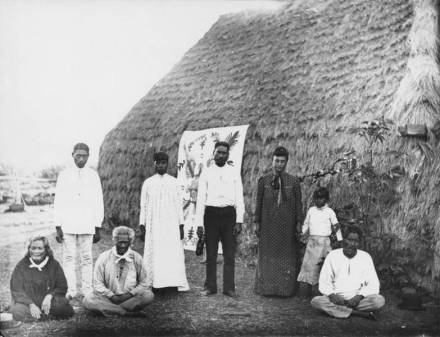
The Quilting Bee (above) shows a community passing along skills, knowledge, and values through an organized tradition. The painter, Anna Mary Robertson “Grandma” Moses (1860-1961), started to paint seriously at age 78, completing The Quilting Bee in 1950. Quiltmaking and quilting bees, also called quilting frolics, were good ways for communities to dispel their situational blues. Quiltmakers have transcended cultures from the earliest known quilts around 3400 BCE in the Egyptian First Dynasty to more recent times in this country. Enslaved Africans, New England Quakers, Hawaiian natives (shown below), and Amish communities in Pennsylvania, Ohio, and Indiana, among countless others, developed quilting expertise, passing along methodologies, and improving the art across generations. [Niihauan quiltmakers, photograph by Francis Sinclair, 1885, Wikipedia.]
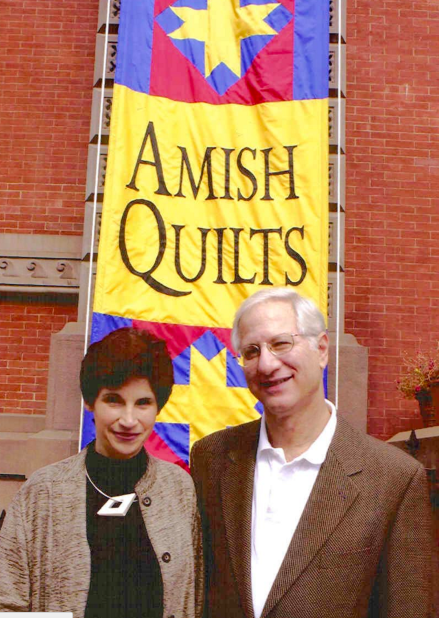
Stephen and Faith Brown, UM alumni and friends of the Urology Department, followed their serendipitous interest to become expert collectors of Amish quilts, exhibiting their quilts at the UM Art Museum, the Renwick Gallery, the University of Kansas, the Denver Art Museum, and the de Young Museum. The unexpected bold colors and patterns of those quilts contradicts the restrained lifestyle of the artisans and surely must have dispelled their blues while enhancing their sense of community. [Exhibit at Renwick. Copyright Faith and Stephen Brown.]
Two.

Succession and success. Skills, arts, and knowledge of quiltmakers, soldiers, archeologists, urologists, and other workers of all sorts survive only through their successors. Virtually every discipline ensures its succession through role-modeling, education, and training, prospering when the processes of succession are deliberate.
At this time of year, medical students are anxiously sorting out their career paths and seniors are taking specialty rotations and applying to training programs. Last year’s seniors are now residents-in-training at Michigan Medicine in the fourth month of what was once called “internship,” currently labeled postgraduate year one (PGY 1) in the jargon and long line of continuing medical education (CME). [Above: Terra Cotta Soldiers of Qin Shi Huang, first Emperor of China, c. 210 BCE. Below: successive UMMS class pictures in UH corridor.]

The Department of Urology, as any recruiting discipline, has the double duty of selling itself to applicants while also appraising them for abilities to succeed in training and practice. Equally important, we want to build our team in urology while enhancing its diversity. We have a strong track record in this work from the days of Program Directors Gary Faerber and Khaled Hafez, and currently Kate Kraft and Sapan Ambani (all shown below).
Gary Faerber (Nesbit alumnus 1989 – now a professor at Duke.)

Khaled Hafez (Nesbit alum 2004)

Kate Kraft (Nesbit faculty 2011)

Sapan Ambani (Nesbit alum 2014)

We had no idea, last year at this time, that interview days wouldn’t take place as usual this season, when digital surfaces will reduce the full human dimensionality day-long experience to constrained transactional computer sessions. Zoom will dominate until society-at-large equilibrates with Covid-19 so we can resume a more human interview process.
Three.
Hopes and dreams. What do residency applicants want? Overall, they want a five-year learning and living experience that will bring them happiness and success, although each individual defines these conditions uniquely.
What do the faculty, current residents and fellows, and staff want? They want bright, industrious, and dependable learners and workers who will be successful in their training and in their careers. From its start in the 1920s, UM Urology has trained people to advance the discipline through care of patients, creation of new knowledge, and teaching of sequential generations. Shared values of integrity, kindness, leadership, and citizenship have been modeled and reinforced in our community of work and learning for nearly 100 years.
For the many applicants to UM Urology, we can offer only a few positions. Selection is necessary, but identification and ranking of top applicants is painfully imprecise. Applicants similarly need to assess the training programs in the national match process and for them as well, no ideal formula, algorithm, set of experiences, or scores, predicts success. Guidance from “experts” at gauging successful outcome is a forlorn hope and appraisal by each party comes down to personal holistic consideration, that is gestalt. During recruiting seasons as department chair, I wished we could have taken many more applicants, as I saw potential for success in training and in life within most candidates. While the matching process is currently an embarrassment of riches for training programs, it is a matter of life-altering consequence for each applicant.

A painting in 1886 called Hope by George Frederic Watts (1817-1904), captures the complexity of the predicament: a blindfolded woman sitting on a globe plays a lyre with only a single string remaining. Possibly she retains optimism in spite of obvious handicaps. Perhaps she is content but realistic. We can only guess the artist’s intent, but regardless of the nature of her thinking and sense of hope, the scene certainly is suffused with the blues. [Above: Tate Museum].
Four.
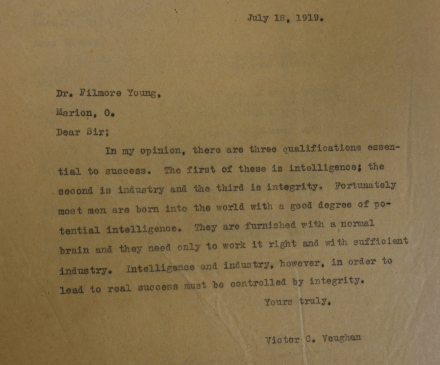
Prediction. The UM Bentley Library contains great riches – we have seen this in our study of the UM Urology history. One exchange of letters between UMMS Dean Victor Vaughan and a physician in Marion Ohio, named Fillmore Young, in July 1919, centered on the question of “Why some succeed, while others fail” in medicine. Young intended to give a paper on the topic and wrote to Vaughan, as “one of about fifteen of the prominent men of our profession who have succeeded,” asking for three indicators of success. As an example, Young quoted three predictors from the prominent American surgeon, Nicholas Senn (1844-1908).
“First: He knew his business.
Second: He asked no outside advice.
Third: He demanded his position.”
Senn’s dogmatic, inflexible, and self-assured advice was ridiculous, largely the antithesis of any responsible advice for success. Vaughan’s reply (shown below) revealed a greater mind and kinder person.
“Dear Sir;
In my opinion, there are three qualifications essential to success. The first of these is intelligence; the second is industry and the third is integrity. Fortunately most men are born into the world with a good degree of potential intelligence. They are furnished with a normal brain and they only need to work it right and with sufficient industry. Intelligence and industry, however, in order to lead to real success must be controlled by integrity,
Yours truly, Victor C. Vaughan.”
Dean Vaughan wrote this just a month after learning of the death of his oldest son, in France at the conclusion of WWI. This was also when Vaughan first considered Hugh Cabot for the chairmanship of the UMMS surgery department, and in whom the qualities of intelligence, industry, and integrity seemed to be in full display.
Five.
Opportunity. One year after this exchange of letters, when the only gender qualified for success in medicine seemed to be male, the 19th Amendment to the Constitution legislated voting rights to women. This doubled the American voting denominator and helped open up the national talent pool for work, ideas, and leadership necessary for society.
While the University of Michigan and its Medical School had been educating women since 1870 and 1871, the numbers of women in the classes, never at parity from the start, sharply dropped off in the first half of the 20th century and only reached parity in the early 21st century. The inclusion of women in medicine doubled the talent pool for medical progress.
More recently, one hopes, the George Floyd tipping point signals a groundswell of sentiment to deconstruct widespread structural racial impediments to equal opportunity for all people to pursue success.
In case you missed Randy Vince’s article, “A piece of my mind: Eradicating racial injustice in medicine,” in JAMA last month, it’s well worth reading. [JAMA, 324:451, 2020.]

Randy, our senior uro-oncology fellow, offers a personal perspective, referring to stages of learning in the transition from ignorance to mastery of a subject. He suggests personal steps to ameliorating social injustice, and the final one, implementation of widespread culturally-aware mentorship training, is predicated on the idea of building pipelines of opportunity for as wide a swath of the human talent pool as possible. This is a matter of widely seeking and extending mentorship throughout all communities of our potential successors. Of course, no single health care provider can mentor every possible community, but a robust team such as UM Urology can probably cover most. [Above: Vince at a socially-distanced coffee break, September 2020.]
Postscript.
Purposes and cross purposes. Higher education is in the news this month, as never before and institutions that figure out how to bring students and teachers together in safe proximity will be highly prized. Hand hygiene, face masks, and social distancing work well. It shouldn’t be rocket science to outfit some classrooms and lecture halls as “test kitchens” with vertical laminar air flow. The reversed air flow need not be “ICU grade,” but just enough to give gravity a little help with respiratory droplets. It would be money well-spent, for this will not be the last pandemic to interrupt educational routines.
Students come to colleges, universities and medical schools for a number of purposes, sometimes cross-purposes. Some want to learn who they are and understand their place in the world. Others seek knowledge and skills, or merely a ticket, to a particular occupation. Many students are deeply curious about a particular subject. No small few simply want liberation from home and opportunities for socialization. Schools, for most students, are a means to some end. G.K. Chesterton, mentioned in these columns last month, once wrote:
“ … in logic a wise man will always put the cart before the horse. That is to say, he will always put the end before the means; when he is considering the question as a whole. He does not construct a cart in order to exercise a horse. He employs a horse to draw a cart, and whatever is in the cart. In all modern reasoning there is a tendency to make the mere political beast of burden more important than the chariot of man it is meant to draw.” (Irish Impressions, 1919)
When the “end-game” is improvement of the human condition, no institution has been more durable than that of higher education in pursuing that object. From times of Socratic and Hippocratic schools to the more formalized educational center of al-Qarawiyyin in Fez (Morocco) in 859 and then Bologna’s “first” university in 1088, and present-day colleges and universities, higher education has aspired to create the citizens, ideas, occupations, and technologies of the future. In a Darwinian sense this is why they endure and grow, yet even complex multiversities, such as UM, remain imperfect in extending their opportunities fully.
We educate medical students and residents to become tomorrow’s urologists, anticipating they will be the leaders and best of urologists. The founder of UM Urology, Hugh Cabot had an even larger view as Medical School Dean, explaining this in 1925 at the 36th annual meeting of the Association of American Medical Colleges in Charleston at the Fort Sumter Hotel October 26-28. His talk “Should medical education be importantly recast?” concluded with this paragraph.
“Finally, but perhaps most important, throughout the whole period of education the goal must be kept in sight, that goal being not the successful practice of medicine but the successful service to the community. If at any point either teacher or student loses sight of service as the paramount object of the practice of medicine, then medicine will fall from its high estate and be classified, and deserve to be classified, as a trade rather than a profession.”
Those remarks anticipated comments made 35 years later on the steps of the Michigan Union by another Bostonian, Senator John F. Kennedy, in a presidential campaign speech on October 14, 1960.
“Let me say in conclusion, this University is not maintained by its alumni, or by the state, merely to help its graduates have an economic advantage in the life struggle. There is certainly a greater purpose, and I’m sure you recognize it. Therefore, I do not apologize for asking for your support in this campaign. I come here tonight asking your support for this country over the next decade. Thank you.”
Hope is tempered by the blues throughout this global village in October 2020, besieged by pathogens, tribalism, extremism of all sorts, authoritarianism, economic challenges, kleptocracy, and environmental deterioration.

Yet, October is still a time for optimism with belief in human ingenuity to fairly share the harvest bounty and solve the problems of our times. When the talent pool for human invention is maximized by including all people, the likelihood of good solutions is increased. The short burst of autumn colors, soon ahead, is one of nature’s best antidotes to the blues before we put on winter clothes, accommodate to the gray skies of Michigan winters, and pull up comforters and quilts at night. [Above: Autumn streets, Ann Arbor 2020. Below: Halloween by Grandma Moses, 1956.]

Thanks for reading Matula Thoughts, October, 2020
David A. Bloom, Department of Urology, University of Michigan