
Michigan Urology Family
[This blog is an alternate presentation of “What’s New” the monthly email newsletter of the Department of Urology, University of Michigan]
Humanity’s new superpower. Declarations of mission, deliverables, & equality. Smiles.
10 items 3038 words

Santa’s sleigh routes. Visualization from the Opte Project of Barrett Lyon, American Internet entrepreneur and artist. This displays the various routes through a portion of the Internet based on opte.org. Each line is drawn between two nodes, representing two IP addresses. The lengths of the lines indicate the delay between two nodes. Lines are color-coded Dark blue: net, ca, us; Green: com, org; Red: mil, gov, edu; Yellow: jp, cn, tw, au, de; Magenta: uk, it, pl, fr; Gold: br, kr, nl; White: unknown.
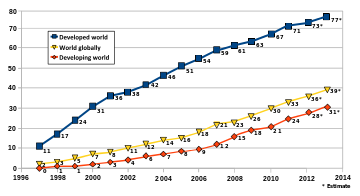
1. With December underway and 2015 just around the corner we are nearly halfway through the fiscal year of 2015. Yet even as we move forward in time history still heavily defines us. On this day, forty five years ago, in 1969 the four-node ARPANET was established (four computer/routers: UCLA, Stanford Research Institute, UC Santa Barbara, & University of Utah), paving the way for the internet without which it is hard to imagine today’s world. The WorldWideWeb was the name of the first web browser (a software application for retrieving, presenting, & navigating information in the form of uniform resource identifiers – URI/URLs) that Tim Berners-Lee created in 1990 using a set of rules to govern the transfer of information between computers. These rules were called the hypertext transfer protocol (HTTP). The browser of Berners-Lee was later renamed Nexus. Soon better competing products appeared – Erwise, Mosaic, Netscape Navigator, Microsoft Internet Explorer, Firefox, Apple Safari, and Google Chrome. Take your pick and enter today’s World Wide Web, our latest information revolution. This so-called digital revolution followed the industrial revolution, which in turn followed Gutenberg’s earlier information revolution of commercial printing. The web is now the digital revolution playing ground with data ubiquity, human connectivity, and computer power translating into “the internet of everything.” The promise of equal access to information should give all people a fair shot at the basic aspirations of civilization – a decent self-determined life affording liberty and the pursuit of happiness, although I don’t see this happening with great speed around the world. The conditions of good government, law & order, food security, health care, education, and personal safety are necessary to ensure all people their due decent life. As physicians, urologists, teachers, nurses, PAs, clerks, administrative staff, and scientists we do our part for mankind’s wellbeing in terms of healthcare, but our attention as citizens to government, justice, and poverty is no less compelling. The internet offers unprecedented opportunity to understand and impact these crucial issues of citizenship. The internet also allows malevolent souls who might be oceans and continents away access to your bank account, personal information, and home thermostat much like an evil Santa Claus entering your life through the chimney of your internet connection. [Diagram – nearly everybody uses the internet: internet users per 100 people. Source International Telecommunications Union]
2. The clinical gaze. The toys of the digital revolution are no substitute for a finely honed clinical gaze. There is no “physician app.” The mandated electronic medical record (EHR) is part of a well-intended effort to bring American health care into the digital age, although most large health care organizations already had effective and meaningful electronic data systems prior to the HITECH Act of 2009. The expensive and clunky systems that satisfy governmentally-defined “meaningful use” and comply with the complex new international classification of diseases (ICD-10) have been a painful adjustment for most physicians and have misdirected their clinical gaze from patients to the patients’ avatars, namely computer screens and keyboards. This misdirection impairs safety and satisfaction. Even though I am not an expert in infectious diseases or Texas hospitals it seems painfully obvious the initial mishandling of the first case of human Ebola in North America was due to a constellation of mistakes, surely including that new avatar. The first and foremost error was the failure to appropriately recognize and react systemically to a sick person from Liberia in September, 2014 when the world knew an Ebola epidemic was spreading out of control. A medical student’s history and physical would have discovered this story, but the dot phrases, templates, pull down menus, and cutting & pasting of the federally-mandated EHR products interfere with the thoughtful acts of looking, asking, and listening to patients. With the computer as the patient’s avatar the human element and fundamental skills of physicians are relegated to the sidelines while the keyboard garners most attention from the doctor in the “encounter.” The systems we are constrained to use obliterate narratives and stories. Those systems are co-conspirators in the Texan tragedy and I have no doubt that many more rookie errors will follow, whether infectious disease-based or not. Somehow it is up to the healthcare professions to mitigate the commoditization and retain the professionalism of our art and science. It would be a shame to lose the clinical gaze that our profession has sharpened and taught over centuries. Stanley Mukundi, a superb Physician’s Assistant in our General Urology Division, pointed out a recent JAMA article by Timothy Daaleman (The quality of mercy, will you be my doctor? JAMA 312: 1863, 2014) that spoke of “administrative waterboarding of prior authorizations, disability determinations, medical leave forms, and the like…” Such is the landscape of contemporary clinical practice, and the legislated EHR has added to the burden for most of us. Whether it be personal political involvement, organizational advocacy, or institutional leadership we each need to engage seriously in the changing face of healthcare to render it effective and safe for patients, as well as attractive in terms of career for the best and the brightest of the next generation.
3. Residency applicants – the next generation. Michigan Urology, I like to believe, is a high performing team, a term we appropriate comfortably from the business world. We are hardly perfect in this sense in Ann Arbor, but as I look around the country we stack up pretty comfortably among our peer urology programs that are generally recognized as the top tier. Thus, it was easy for us to “sell” our training program and our mission as we met with the 63 candidates elected for interview from 340 applicants. No doubt we missed some other great candidates, but the amazing individual accomplishments, the high scores, great letters of recommendation from our colleagues, and our own time constraints mandated a line of demarcation between those we interviewed and those left behind. Without question, the medical students who want to become the next generation of urologists are the sharpest we have ever seen. The next step in the process is for us to make a list of those we want to join us – from number one to number 40 or so. The candidates make similar lists for themselves and then a computer sorts things out. We usually end up with 4 out of our top ten as many factors weigh into their individual decisions. For some candidates, family proximity or job of a spouse (or fiancé or significant other) may favor or disfavor an Ann Arbor location. In another 2 months I should be able to tell you who will comprise our class of 2020.
4. Mission. A highly performing team has to keep the idea of its mission firmly centered in the workplace and in the minds of its members if it is to remain a high performer. Our mission in the Department of Urology is focused on health care: teaching it, doing it, and making it better. We had a recent discussion of our mission at a faculty meeting and Jeff Montgomery suggested a single word change to get rid of some redundancy and to improve clarity of our mission statement. That involved using the word clinical instead of quality thus leaving the following mission statement: The University of Michigan Department of Urology exists to relieve urologic disease & disability by providing exceptional clinical care, training future leaders in urology, & expanding urologic knowledge through research, innovation, & collaboration. The value in articulating a clear mission statement in language that fits the day, is to understand the reasons for existence and the goals of the organization and then to unite them to the aspirations of its stakeholders.
5. Essential deliverable. The essential deliverable of any organization may not exactly be the same as its mission. The mission statement tells why an organization exists, while the essential deliverable refers to its primary product. You could argue that our essential deliverable is the next generation of urologists and scientists, or that the main deliverable is the next iteration of knowledge in our field. Accountants might narrowly argue that the primary deliverable of our urology department is bringing money to a health system. The real story is this: we have a mission of three main parts: educating the next generation, growing the knowledge base of urology, and delivering high quality state of the art urologic care. This last mission facet provides the essential milieu for the first two aspects of our mission. Furthermore, it becomes the moral priority, the epicenter of the organization, because the demands of clinical care (so often unexpected) at any given moment trump all other duties. The art of our work, however, is achieved in building the teaching and research around clinical urology. Our essential deliverable is “Kind & excellent patient-centered care, thoroughly integrated with education & innovation at all levels.” We developed this phrase over the past few years and some of the faculty find it compelling enough to include as a sort of declaration of our department, on their routine correspondence. The electronic medical records, deemed appropriate and meaningful by recent federal regulation, now relegate the essential transaction to a business-like encounter. In fact the doctor-patient interaction is currently called an encounter. What do patients want from these encounters? Speaking as a patient I hope for expertise, kindness, and convenience, in that order. For me, as a healthcare provider (physician), mastery, autonomy, and meaningful purpose are the main drives (and I credit Daniel Pink’s book, Drive, for helping me articulate those desires).
6.  Our Declaration. Speaking of declarations, as you contemplate some holiday time ahead, free from the demands of schedules and obligations, one book worthy of your attention is Our Declaration by Danielle Allen. This provides a lively study of the historical context and a deep analysis of the meaning of the Declaration of Independence. The author makes a strong case that the Declaration does not establish a competition between the values of liberty and equality as many people have assumed. The two attributes do not play off each other to create a zero sum game; liberty does not exist at the expense of equality or vice versa. Rather Allen believes that equality is a necessary condition for liberty in a democratic society. Her understanding of equality, however, was far more sophisticated than mine before I read her book. As citizens enjoying the blessings of a free society and as teachers in a great public university, it is our duty to be literate in the underpinnings and structure of our national situation.
Our Declaration. Speaking of declarations, as you contemplate some holiday time ahead, free from the demands of schedules and obligations, one book worthy of your attention is Our Declaration by Danielle Allen. This provides a lively study of the historical context and a deep analysis of the meaning of the Declaration of Independence. The author makes a strong case that the Declaration does not establish a competition between the values of liberty and equality as many people have assumed. The two attributes do not play off each other to create a zero sum game; liberty does not exist at the expense of equality or vice versa. Rather Allen believes that equality is a necessary condition for liberty in a democratic society. Her understanding of equality, however, was far more sophisticated than mine before I read her book. As citizens enjoying the blessings of a free society and as teachers in a great public university, it is our duty to be literate in the underpinnings and structure of our national situation.
7. Equality. Everyone deserves a fair shot at a decent self-determined life. This is the basic presumption of equality. Allen suggests equality consists of 5 main aspects: a.) no domination – equality of presence & opportunity; b.) equal access to government and laws; c.) equality in contribution to collective intelligence (everyone’s opinion matters); d.) equality of practices of reciprocity (this one is a key point – the balancing of agency in human relations, that is the mutual ability to recalibrate or redress imbalances in encroachments of freedom); & e.) equality of ownership of public life. Recently I thought another facet of equality should be considered – the equality of recognition. This idea came to mind as I read about an American woman who became involved in terrorist activities and was tried in court wearing a burka that covered all of her face but her eyes. Facial recognition and facial expression are essential elements of society and human communication. While in a free society people should be able to dress and worship as they like, if they want to engage in public civil and legal rights, they must represent themselves on an equal basis with their fellow citizens. No subset of society should have a general right to concealment. As I studied Allen’s 5 main facets of equality, however, I came to appreciate their sophistication and realized that the point of recognition equality is not separate from but intrinsic to each of the 5 aspects that she carefully explains. Equal access to information (data ubiquity) is also fundamental to all of the equalities that Allen describes.
8. The fragile human condition. It’s too soon to forget about Ebola, and even if it fades for now it is just one more example of humanity’s recurring deadly threats, notably infectious diseases of micro-organisms and social epidemics of the human mind whether the latter are the Crusades, the medieval inquisitions, communism, Nazism, McCarthyism, or Middle East extremism. Once viewed as an exotic problem with improbable global spread, Ebola is now part of the daily conversation of practically every emergency department on the planet, having joined the roster of global threats. Paul Farmer wrote an interesting piece on Ebola in Liberia [London Review of Books 23 October 2014] and made this well-informed claim. “An Ebola diagnosis need not be a death sentence. Here’s my assertion as an infectious disease specialist: if patients are promptly diagnosed and receive aggressive supportive care – including fluid resuscitation, electrolyte replacement and blood products – the great majority, as many as 90 percent, should survive.” Comprehensive national health care, sadly lacking in much of western Africa, is a basic expectation for any competent state or nation. Equal access to basic health care, a pre-condition for any civilized modern society, should have been by now one of the essential fruits of these great “revolutions” of humanity – the industrial and the informational.
9. Burghers. One might describe citizens of the world as burghers, a term that once implied a comfortable existence. In fact, all citizens of the world deserve comfort. As technology brings new superpowers, such as the internet, to humanity and the tribal village emerges into a global village, good government becomes even more paramount to global security, individual safety, equality, and freedom. Although far from perfect, the United States of America has gotten government about as good as it has gotten so far. All nations, however they construct themselves, must bring their governments closer to a basic standard of effectiveness and fairness if humanity is to endure. Failed nations, such as we see in Africa, the Middle East, and other places surely cannot continue to fail without bringing down the rest of the planet. Ebola is only one tiny and hopefully transient, example. The challenges of political leadership perpetually perplex humanity. I was reminded of this a few months ago in Washington DC at the Hirshhorn Museum when passing a cast of Auguste Rodin’s sculpture, The Burghers of Calais, commissioned in 1884. This was intended as a monument to an event in 1347 during the Hundred Years’ War when that French port was under siege by the English. You can read the story of the siege in Wikipedia, but the anguish that Rodin depicted in the burghers of Calais is a universal one seen century after century by our parents, grandparents, and great grandparents back through time. The self-inflicted wounds of humanity are sadly self-inflicted. Transgressions against equality, freedom, and the right to decent self-determined lives repeatedly overpower the new superpowers we accrue.

[Burghers of Calais, Smithsonian Museum/Hirshhorn Sculpture Gardens on a bright sunny day in Washington, DC, August, 2014. Curiously, French law allegedly decrees that no more than 12 casts of any Rodin work can be made. The original version of the Burghers in Calais was cast in 1895. The Smithsonian/Hirshhorn sculpture was cast in 1943 and you can find other casts near the Houses of Parliament in London, the Rodin Museum in Philadelphia, The Norton Simon Museum in Pasadena, the Metropolitan in NYC, the Kunstmuseum in Basel, and others in Copenhagen, Belgium, Paris, Tokyo, and Seoul. Stanford has sculptures of the individual figures, no doubt skirting the letter of the French law.]
10.  The burghers of Calais reflect the faces of anguished citizens in far too many parts of the world. Perhaps 2015 will be the year we start to straighten out ourselves as a species, but come what may I expect the highly performing team of the Urology Department here at the University of Michigan will be doing its part in pursuit of its missions and essential deliverable. Tomorrow is our departmental holiday party, one of my favorite events of the year, where we will see 250 or more Michigan Urology “burghers” and many of their children. Smiling children beat grimacing burghers any day. The ultimate missions and essential deliverables for all global citizens today should be targeted to maximizing the smiles of the next generation. Happy December and best wishes for a good 2015.
The burghers of Calais reflect the faces of anguished citizens in far too many parts of the world. Perhaps 2015 will be the year we start to straighten out ourselves as a species, but come what may I expect the highly performing team of the Urology Department here at the University of Michigan will be doing its part in pursuit of its missions and essential deliverable. Tomorrow is our departmental holiday party, one of my favorite events of the year, where we will see 250 or more Michigan Urology “burghers” and many of their children. Smiling children beat grimacing burghers any day. The ultimate missions and essential deliverables for all global citizens today should be targeted to maximizing the smiles of the next generation. Happy December and best wishes for a good 2015.


[Santa & the children of Michigan Urology at Fox Hills, December 2013; Sheryl Lucas from Mott Surgery/Urology ACU and children]
Michigan Urology Soundbites. Professor Brent Hollenbeck was inducted into the U of M Medical School League of Research Excellence. Assistant Professor Daniela Wittmann has received a 1.6 million dollar award project as principal investigator for 3 years focused on sexual recovery after prostate cancer treatment funded by the Movember/Livestrong organizations. David Miller announced that “Chad Ellimoottil, our NIDDK-T32 Health Services Research (HSR) fellow currently away for the year at Loyola University in Chicago, received a one year Urology Care Foundation Research Scholar Award for ‘Medicare Payment Variation for Kidney Transplantation: Implications for Episode-Based Bundled Payments.’ Chad’s proposal was selected from among 48 applicants, and this prestigious grant reflects the quality of his work and his potential for a career in academic urology and HSR. We look forward to having him return to Ann Arbor in July.” Last month our internal weekly “What’s New” profiled: a) two new faculty: Nick Warner specializing in reconstructive surgery at the VA and Jim Dupree specializing in andrology/infertility, b) a Pediatric Urology Update by Julian Wan, and c) “What’s New” in the Taubman ACU by John Stoffel. Website: http://www.med.umich.edu/urology/about/MonthlyNewsletter.html.
Thanks for spending time on “Matula Thoughts.”
David A. Bloom
