
WN/MT 3 April 2020
2356 words
This April, perhaps the cruelest month


One.
April, was the original title of this painting by American impressionist Frederick Childe Hassam, a century ago, in 1920. It was an optimistic time when the world was rebounding from years when the thin veneer of civilization seemed to be wearing away with war and influenza. The pendulum of events changed for the better and, in Ann Arbor, Hugh Cabot started up a century of modern urology at the University of Michigan.
It is a mystery what drove Hassam, just then, to go back to his very beginnings with this work. Maybe the emergence of the world from the edge of catastrophe just then was a factor. He renamed his painting, Green Gown, the woman in green being Rosa Delia Hawthorne, Hassam’s mother, depicted in an April a half century earlier when three months pregnant with Frederick (born October 17, 1859 in the family home in Dorchester, Massachusetts). [Above: April, Courtesy, Gibbes Art Museum.] The gorgeous composition shows Hassam’s imagination of his mother at 27 years of age, reclining pensively on a settee, as if considering her next 6 months of confinement or the joys and trials of parenthood. A daffodil arrangement in the right foreground reinforces the time of year in the original title. Yet it was an odd concept for a painting, with the artist picturing his mother in the first trimester of pregnancy with him, at his actual beginning. This was a curious contrast to Whistler’s famous consideration of his own much older mother a half century earlier.
Hassam’s painting is a suitable introduction to April, the beginning of spring in the northern hemisphere, when showers anticipate May flowers, as the saying goes. Another painting by Hassam, The Avenue in the Rain (in the White House Collection) depicts Fifth Avenue in NY around the time of WWI and perhaps during some April showers. This was one of 30 paintings in Hassam’s Flag Series.

Hassam purchased a home in 1919 in East Hampton where he most likely painted April the following year and would live another 15 years, dying in East Hampton at a respectable 75. The country was in a patriotic mood in April, 1920, with the Great War and recent influenza epidemic no longer existential threats, but the national optimism eclipsed any prudent attention and resources to prepare for the next iterations of existential threats. This April, normally a time for beginnings, existential threats are back at civilization’s door. [Above: The Avenue in the Rain. Hassam, 1917. White House Collection, since the Kennedy Administration. Below: Oval Office 2009, photo by Pete Souza with the president and the picture on the wall.]

Two.
A century is a convenient milestone, although most humans fall short of this in their life spans. The modern average of “three score and ten” or so, however, is ample time to leave something behind, if one is fortunate, in good works, successors, and kindness. Octogenarians, septuagenarians, and centenarians are rarities, the products of good genes and lucky circumstances. The U.S has 80,000 centenarians, the U.N. estimates 343,000 worldwide in 2012 and projects 3.2 million by 2050.
A century is an extreme stretch for a single human, few make it that long, but human collectives – nations, organizations, corporations, and other teams – are not limited biologically and for them a century is a useful ruler to measure accomplishments and create historical narratives. So, consider medical practice and urology in April 1920, in particular, when the grim experiences of war and influenza were fading from memory, although some lessons learned were working their way into civilian health care. The growing scientific knowledge base of medicine and its burgeoning subspecialties by 1920 had rendered medical school alone insufficient training for the new generation of medical practitioners; internships and residency programs were producing a new world of graduate medical education that became the career-defining element of medical training.
This centennial year of urology at the University of Michigan is an opportunity to understand our organizational corporate past and some of the many stories relevant to Michigan Urology. Additionally, the centennial is a chance to personally reconcile with our roots in healthcare and at the University.
With the present world turned upside down by Covid19, the AUA in Washington, DC and Sunday Nesbit reception are cancelled, but we look forward to the autumn and September 24-26 with the Nesbit alumni reunion here in Ann Arbor, featuring guest speaker alumni Carol Bennett, Barry Kogan, Ananias Diokno, Carl Smith, Curtis Nickel, Mitch Albom, and Sherman Silber, among others. The first of our two books on Michigan Urology will soon be available (and also online via Michigan Publishing), this being Urology at Michigan – The Origin Story, tracing the development of genitourinary surgery, the University of Michigan, its Medical School, and the introduction of modern urology to Ann Arbor by Hugh Cabot. Book two will cover the first hundred years of urology at Michigan, year by year, expanding on the Konnak and Pardanani text that Jim Montie commissioned 20 years ago. We hope to finish this in the next year.
This April 2020 it’s natural to pause for a moment and consider what urology practice and education were like 100 years ago. Cystoscopy, a new skill of the late 19th century, required special instruments and novel expertise that defined urology and fueled its early creative burst. A new breed of surgeons picked up cystoscopy, improved the technology, gained insight into genitourinary dysfunction, and created miracles of minimally-invasive therapy. Nonoperative and open solutions to urinary problems expanded urology, after it was so-named in 1902. Urology came together as an open organization in 1910, created rational training programs for young physicians, and formed its own journal in 1917. Little of this progress translated to the battlefields of WWI, but the civilian progress accelerated after its conclusion, although barely in time to be applied in the next war.
Three.
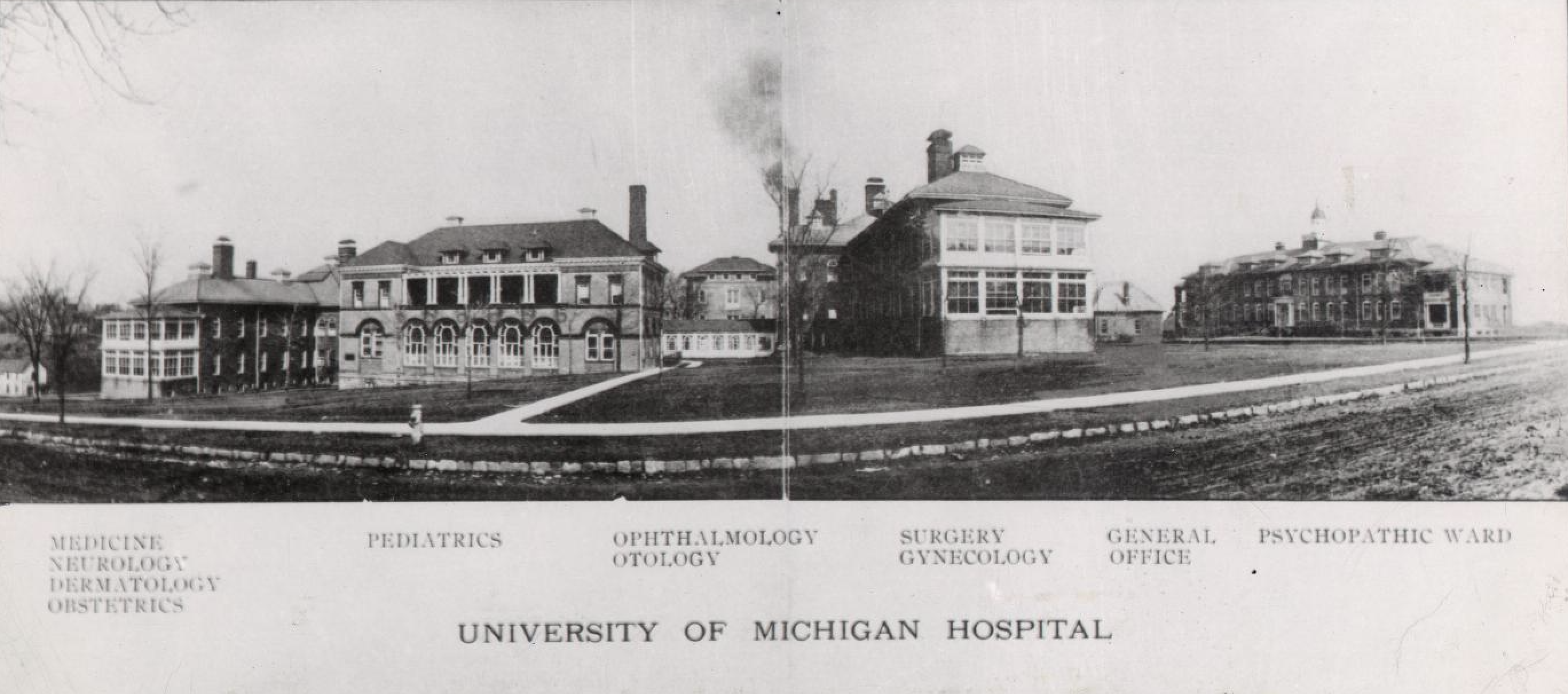
In April, 1920, the Cabots were adjusting to their new lives in Ann Arbor. Hugh was busy as chair of the Surgery Department and the sole urologist at the University of Michigan. Cabot’s two competitors in Ann Arbor, still calling themselves genitourinary surgeons, had left the university to practice a few blocks away at St. Joseph’s Mercy Hospital and neither they nor Cabot had any interest in collegial relationship. The University Hospital complex was physically constrained and outdated, pale in comparison to the facilities Cabot left behind in Boston, but a quantum leap from the 2,500-bed hospital he had commanded in France on the Western Front of the Great War.
The Cabot family was living temporarily in the President’s House, having cajoled the Regents into its use pending the anticipated summer arrival of incoming President Burton. Anxiety was growing within the university administration as it tried to coordinate renovations demanded by the Burtons and uncertainty over the Cabot’s plans. At work, Cabot had to manage the teaching and clinical responsibilities of his small Surgery Department, deploying the full-time compensation model. To grow his small and inbred Surgery Department Cabot leveraged his military connections to bring two essential additions to Michigan that year, Frederick Coller and John Alexander.
Four.
Just about halfway between the start of the Michigan Urology centenary and now, I began my era of training. It was 1971 and urology was at a watershed. It sat between an era of board-certified urologists with life-long certification working in individual or small practices and the present era of urologists with contingent re-certification working in large practices or multispecialty health systems. In 1971 fiberoptic cystoscopy had only recently replaced first generation cystoscopes, illuminated by distal mignon lamps of Edisonian technology; transurethral surgery was one of surgery’s rare minimally-invasive operative procedures; major open reconstructive urologic procedures were available at only a few centers; the intravenous pyelogram and retrograde injection studies were the main imaging modalities (ultrasonography was in its primitive stages); and training programs were mostly small and weakly standardized. That year, Jack Lapides Section Head of Michigan Urology from 1968 through 1983, introduced his strongly disparaged idea of clean intermittent catheterization.
Meaningful visual cystoscopic acuity for old-time urologists required much skill, art, and experience. For learners, peeping over the shoulder of cystoscopists (whenever they decided to let learners have a look), the opportunity was fleeting. This scenario earned Jack Lapides his covert nickname, Black Jack: for he was known to temporarily disconnect the light cord (by stealth of hand) before letting the learner look through the scope and asking what they saw. [Below, Jack Lapides photo by DAB.]

Lapides had been a loyal and productive lieutenant to Reed Nesbit for some 20 years. When Reed was aiming toward retirement in 1967, Jack no doubt felt inclined to take over the leadership of the small section. The two urologists seemed to have gotten along well professionally, although there was no doubt as to who was in charge and it didn’t seem that a strong friendship existed outside the workplace. Lapides had been running his own separate and independent residency program at Wayne County Hospital, graduating a single chief each year whereas at this point the UM program was finishing 2-3 per year.
Karl Montague (UMMS 1968), visited by us last autumn at the Cleveland Clinic, recalled his experience as a junior medical student rotating on urology. Karl had been focused on a career in cardiology, primed in that direction by an NIH fellowship in Basel, Switzerland. Urology at the University of Michigan was then a mandatory clinical rotation and Montague recalls some of Lapides’ pedagogical antics (at the VA):
“Dr. Lapides was demonstrating cystoscopy to a group of us medical students in our third year. Of course, this was before the time of video teaching and the learner had to peer over the shoulder of the teacher who had positioned the scope over a landmark view of anatomy or pathology, while the patient was under anesthesia as happened to be the case that day. So Dr. Lapides had the first student in turn to look in the scope and asked: ‘Do you see the verumontanum?’ The student, after a few awkward moments said ‘Yes’ and Lapides checked the position and asked the next student, who again agreed. When it was my turn, I looked and looked and finally said ‘No.’ It turned out that the Professor was holding the scope in the middle of the full bladder, nowhere near the veru. He seemed to like me after that day and later in the rotation asked my career plans. I told him it was cardiology. He said: ‘Think about urology, and if it interests you, come back and talk to me.'”
Montague did give some thought to urology and that changed his career arc and life. It was a clever and kind approach on the part of Lapides, kinder than the anecdotal “Black Jack” stories. [Below, Montague in his office at Cleveland Clinic, autumn 2019.]
Five.

Kindness & Kurt Vonnegut Jr. (November 22, 1922 – April 11, 2007). The Vonnegut books I read in college, medical school, and during residency offered great escape from study with humor, satire, and surreptitious insight into the thing we call, the human condition. More than appreciated at the time, Vonnegut expanded my sensitivities to the comorbidities of life, environmental deterioration, and the quality of kindness. Cat’s Cradle (1963), iconic book, offered very short chapters that fit my short extracurricular attention span. [Above: “Two Young Women Seated playing cat’s cradle.” Suzuki Harunobu, ca. 1765. Wikipedia.] Slaughterhouse-Five (1969, film 1972) didn’t mean so much to me then, but years later hearing a beautifully performed audiobook, I felt its powerful impact, reflecting Vonnegut’s lived experiences as a prisoner of war in the Allied firebombing of Dresden. Even though I served in a peacetime Army for four years after my residency training, I had gained enough maturity, experience, and knowledge to appreciate that mind-bending book.
Vonnegut told stories of contrived odd characters and places. While exaggerated and even preposterous, he resonated with the best and worst of human attributes. God Bless You Mr. Rosewater (1965) only came recently to me, as I was tracking a quote that reflects Vonnegut’s dark humor and the hope that underlies his satire. The quote came from an anticipated baptismal greeting:
“Hello babies.
Welcome to Earth.
It’s hot in the summer & cold in the winter.
It’s round & wet & crowded.
On the outside, babies, you’ve got 100 years here.
There’s only one rule that I know of, babies –
God damn it, you’ve got to be kind.”
T.S. Eliot once called April “the cruelest month” so it seems fitting to conclude now with thoughts of kindness, a trait that seems to come naturally to some people, but most of us have to work at it, balancing it against our selfish particularities. Kindness is a very human trait, the very basis of civilization, although many other creatures evidence kindness in numerous ways. Kindness is, no doubt, tied into mirror neurons, oxytocin, and other incredible biologic inventions that we are dimly aware of at best. Motherhood is the ultimate expression of kindness, perhaps that was on Hassam’s mind to some extent in April, 1920.
Postscript.

With few centurions living today, only historians can tell us much about what daily life was like during the big influenza epidemic of 1918-1920 that ended around the time Michigan Urology’s first century began. And, of course, one hundred years from today, will many people fully understand the anxieties, terrors, and tragedies of the present moment in time.
Kindness is always at risk in the busy workplaces of healthcare, and this will be especially tested in this current pandemic threat (Coronavirus 19), that has taken civilization by surprise. We are too often surprised by infectious diseases, whether cyclic or novel and while our immune systems may be surprised, our brains have no excuse. Here is an amateur historian’s list of the last big pandemics:
HIV/AIDS rising from 1976 to 1981 and peaking 2005-2012, killing 36 million
Influenza H3N2 1968 killing 1 million
Influenza H2N2 1956-58 killing 2 million
Influenza H1N1 1918-1920 killing 20-50 million
Sixth cholera pandemic 1910-1911, killing somewhat under 1 million, estimated.
Influenza H3N8 1889 – 1890 killing 1 million
Third cholera pandemic 1852-1860 killing 1 million
Black Death (bubonic) 1346-1353 killing upwards of 200 million
The Plague of Justinian (bubonic) 541-543 killing up to 25 million
[Above: Red Cross volunteers assembling gauze face masks at Camp Devens, MA, 1918.]
Thanks for reading Matula Thoughts this April, 2020. It will be a rough month.
David A. Bloom
Department of Urology
University of Michigan
