Matula Thoughts Jan 4, 2019
Sun rise 2019
3734 words

Periodic re-explanation. This column, Matula Thoughts, recalls ancient uroscopy flasks called matulas, used for centuries to examine urine for clues to illness. People want to know “what comes next,” a question, explicit or unspoken, dominating most conversations in medical practice: “can it be fixed and what will happen to me?” Remedy and prognosis mattered more than diagnosis in ancient days, when technology and verifiable medical knowledge were sparse, and understanding pathophysiology (using today’s terms) was not as useful to a patient as remedy and prognosis. Direct examination of urine, particularly for color change, was one of the few early tools of practitioners and the matula was the dominant symbol of the medical profession for over 600 years in western art, until Laennec invented the stethoscope in 1816.
As a monthly collection of thoughts, relevant and random, from a senior genitourinary surgeon, the title seems appropriate. This electronic column began nearly 20 years ago in Allen Lichter’s dean’s office as a weekly email called What’s New. After returning full time to Jim Montie’s Urology Department in 2007, we continued What’s New as a weekly communication, published every Friday by varying members of our department, except for the first Friday of each month when I claimed the electronic podium. A parallel version began 5 years ago on the website MatulaThoughts.org. Happily, the Department of Urology will soon have a new chair with forms of communication to better match the times and people of the next decade. Nevertheless, this monthly habit will continue at MatulaThoughts.org reflecting personal observations, relevant and irrelevant, and events related to Michigan Medicine and the Department of Urology. [Above: Sun face on ceiling fresco, church of Saint Jean-Baptiste de Larbey, Southwestern France. 1610. Wikipedia. Below: variant of Nesbit log by Julian Wan.]
One.

Imagine just 100 years ago how different things were for our predecessors at the University of Michigan Medical School: Americans were recovering from WWI and the first two deadly waves of the 1918 influenza epidemic; Woodrow Wilson was US president, having been Princeton president when he was offered the Michigan job ten years earlier; women couldn’t vote and any adult could drink alcohol on this day in 1919, but by the end of the year women’s suffrage was secured in the 19th Amendment and prohibition came with the 20th Amendment; socialist and communist parties were on the rise; anarchists were preparing for spring bombings; and racial tensions festered nationally. Meanwhile, the University of Michigan carried on with its work at the Medical School and University Hospital, as life went on in Ann Arbor. [Above: Approaching New Year’s Eve, December, 2018, Liberty & Ashley, Ann Arbor.]
The University in 1919, already more than a century old as an organization and in Ann Arbor for around 80 years, was amidst a building binge under President Hutchins with the new Union, Art Museum, Hill Auditorium, and other defining structures. The 60-year old Medical School, which had looked quite good to Flexner on his visit in 1909, had since fallen behind its peers in terms of facilities. The hospital was badly out of date well before the war and replacement was further delayed by the national emergency. The practice of urology at UM was a little more than a single faculty effort in a surgery department consisting of a handful of other individuals.
Late in 1919, Medical School dean Victor Vaughan recruited Boston urologist Hugh Cabot, who would engineer 11 years of change bringing the Medical School back to the top of medical education internationally and at the pinnacle of state-of-the-art clinical practice for the first time. Academic urology in Ann Arbor surely began with Cabot.
Two.
Pundits and ordinary folk made predictions and resolutions when the sun rose on 1919 and we repeated these customs three days ago. Events will happen and paradigms will surely change over the next 12 months, but the only solid predictions this posting will offer for 2019 are: a new chair will begin stewardship of this fine Department of Urology sometime soon and we will celebrate the Michigan Urology Centennial later in the year. Other than those predictions, the rest is noise (to borrow the title of the book on 20th century music by Alex Ross). Sunrise each new day or year brings uncertainty and new possibilities. Predict and resolve whatever you wish, paradigm changes are usually outside your control, although the ability to recognize their inflection points is a useful gift. [Below: Encyclopaedia Biblica, 1903. Public domain.]

The centrality of the Sun to life is a fundamental feature of biology and logically a universal symbol in human civilizations. The 14th century BC image of pharaoh Akhenaten (Amenhotep IV) worshipping sun god Ra, in form of Aten, shows a partial solar disc with rays ending in little hands. Curiously, Akhnaten (1983) was one of three biographical operas written by American composer Philip Glass, the other two being Einstein on the Beach (1976) and Satyagragha (in 1979, about Mahatma Gandhi).
Inevitably, an Anthropocene imprint was added to the sun, seen in the introductory figure from Larbey and much earlier in a 4th century BC marble relief of sun god Helios driving his chariot at the Temple of Athena in Troy. [Below: Pergamon Museum, Berlin.]
The man-in-the-moon, a whimsical anthropomorphic imagination, when combined with a solar face suggests the ancient Asian complementary opposites yin and yang. [Below top: Amiens, Bibliothèques d’Amiens Métropole, manuscrit Lescalopier (Fourth Day of Creation) c. 1200. Wikipedia. Bottom: yin and yang.]

Janus, Roman god of beginnings, looked to both the future and the past, presiding over transitions such as war and peace, and might be viewed as a symbol of paradigm shifts in modern times . [Below: Janus, Vatican Museum.]

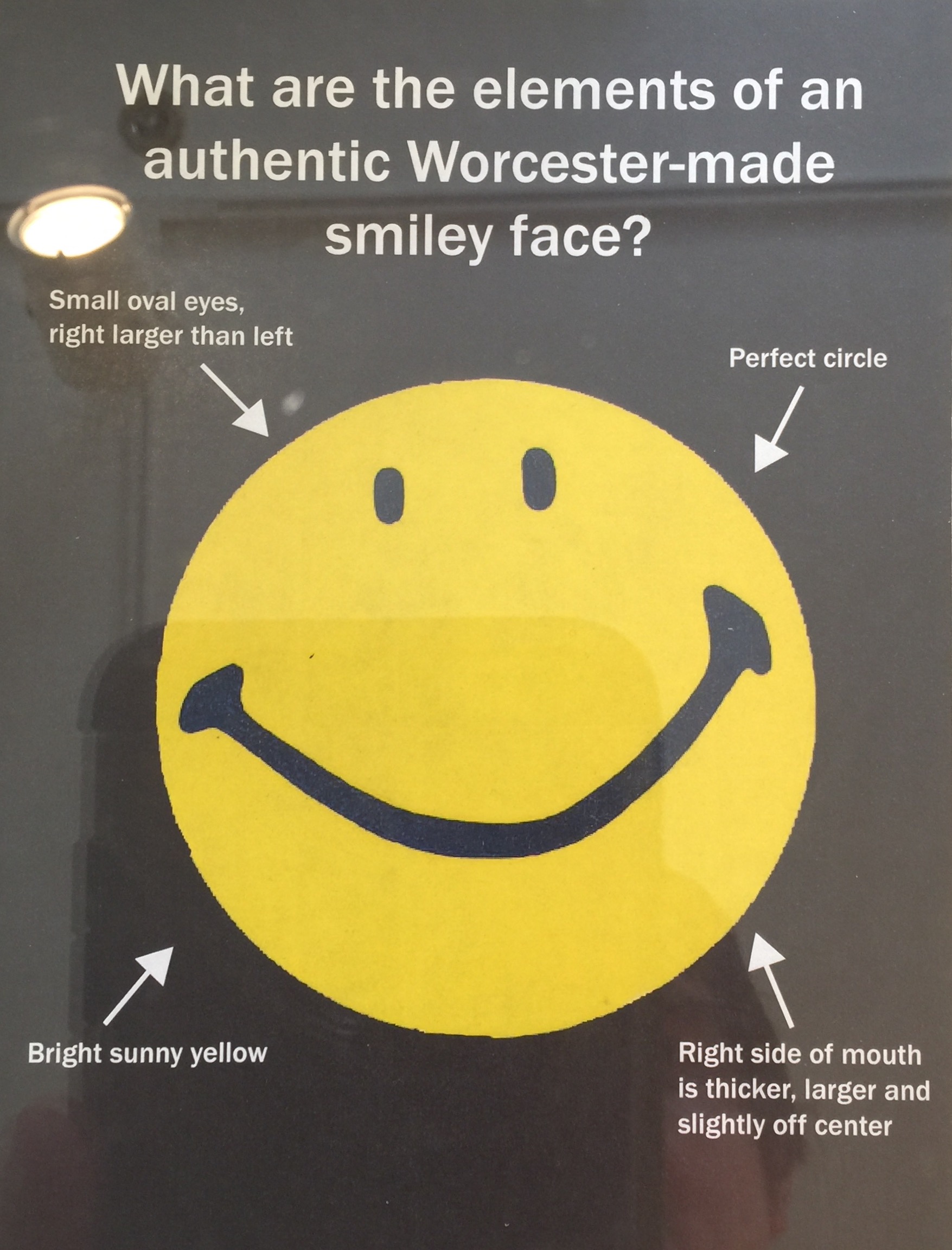
Solar symbols, seen on some national flags, are ubiquitous in the Happy Face, the mother and father of all emoji, designed by commercial artist Harvey Ball in 1963. Charles Kuralt’s Sunday Morning show, launched by CBS News on January 28, 1979, continues to employ a solar disk theme throughout 40 years of reiteration by Charles Osgood and Jane Pauley, remaining a pinnacle of news and civilized commentary as each episode rolls through a set of beautifully curated solar symbols. [Below: Sunday Morning (top) & Authentic Worcester Smiley (bottom).]

Three.
Isaac Newton’s big paradigm shifts began inauspiciously when he was born this day in 1643. His birth date in the old-style calendar was 25 December 1642, but Gregorian conversion brings his birthday to today in the modern calendar and solar year. Bad luck shaped him from the start; father died three months before he was born and mother commented that Isaac, ar birth, could fit inside a quart mug (Wikipedia). Mother remarried, but young Isaac, unhappy at home and bullied at school, reacted by focusing on his studies, becoming a top student at Trinity College in Cambridge. Apples, gravity, planetary motion, and mathematics come to mind at first with Newton’s name, which is also celebrated in the term for a unit of force.

Newton’s color theory was another product of his astonishing ability to think about the world and find clarity about how things work. Countless people before him had seen white light refract through glass prisms into the colors of the visible spectrum and everyone sees rainbows. Yet only Newton carried those observations into a theory of color, described in a book he wrote at 71 years of age in 1704: Opticks: or, a Treatise of the Reflections, Refractions, Inflexions, and Colours of Light. [Above: double Alaska rainbow. Eric Rolph. Below: Color wheel of Goethe. Wikipedia.]
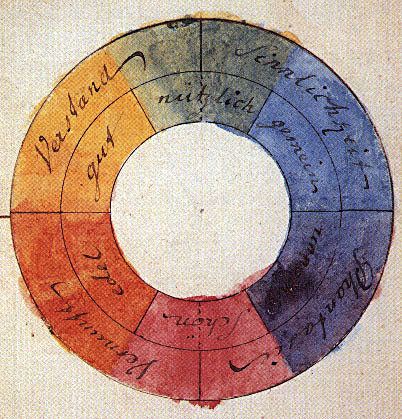
Color theory continued to attract great minds, including German polymath Johann Wolfgang von Goethe (1749-1832) and Scottish scientist James Maxwell (1831-1879) whose differential equations in 1865 explained the electromagnetic spectrum. [Below, User:penubag, Wikipedia.]


An early Apple Computer symbol (above) was perhaps an intentional play on Newton himself and Adobe’s color disk (below) fragments color into infinitesimal gradients of hue.
Four.
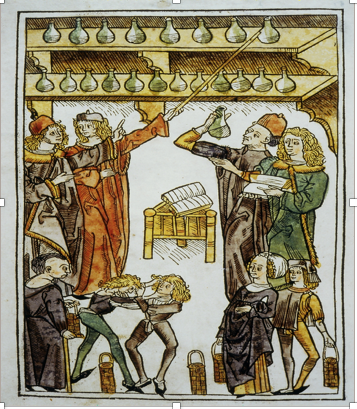
Urine may not be a window to the soul, but it’s a useful indicator of disease through color, sediment, or odor. Red is an obvious hallmark of trouble, whether renal trauma, urinary stone, kidney cancer, bladder cancer, infection, BPH, structural anomaly, metabolic dysfunction, rhabdomyolysis, or genetic mutations. Ancient uroscopists expanded color change into fanciful imaginations and medieval uroscopy charts offered wild speculations of what color, sediment, consistency, smell, and taste of urine might portend in terms of prognosis. [Below: uroscopy clinic. Hortus Sanitatis. 1491, Mainz. Courtesy Dick Wolfe, Countway Library.]
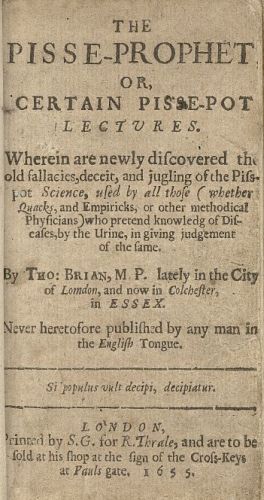
The paradigm shift from uroscopy to urology occurred over two centuries replacing sensory examination of urine by eye, nose, and occasionally tongue, with microscopy and chemical analysis. Nevertheless, persistent uroscopic fortune-tellers claimed legitimacy even in the face of emerging scientific reason. Thomas Brian’s book in 1637, The Pisse Prophet, is a classic example of rational attempts to debunk dogma and fraud.[Below: Wellcome Library, 1655 copy.]
The metabolic dysfunction porphyria (named for purple urine) affected Scottish physician, Archie Cochrane, born 110 years ago in 1909 on January 12, and the prime advocate in modern times for evidence-based health care. Later this month Guilia Lane, our FPMRS fellow, will educate us on Cochrane in What’s New. [Below: normal urine sample on left and porphyria sample on right.]

This sample below from my clinic a few years ago was oddly green, but I failed to make note of the cause. Color still matters in modern urinalysis although, since matulas gave way to microscopy and chemical analysis, physicians rarely demand to view urine themselves before it heads to a machine or laboratory.
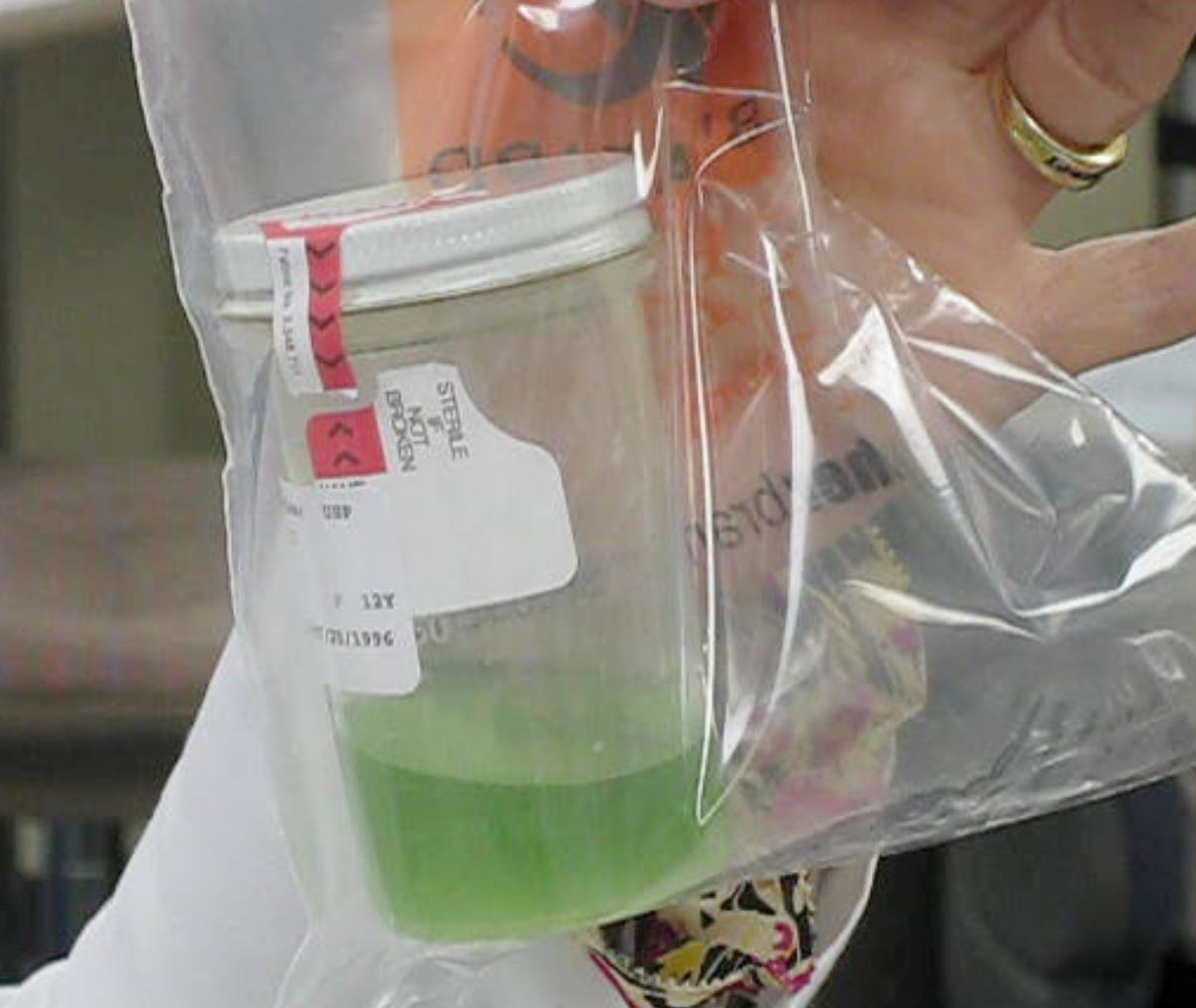
Macroscopic uroscopy gave way nearly completely to modern urine investigation with specific gravity measurement, chemical analysis, microscopic exam of spun sediment, bacteriologic culture, antibiotic sensitivity testing, and who knows what will come next. Twentieth century urinalysis was a cornerstone of urologic practice when it was unimaginable for a patient to leave the office of a good urologist without submitting a urine for examination. Hinman’s Eight Steps to Presumptive Diagnosis constituted the basis of urologic practice, at his start in San Francisco in 1920 as the first trained urologist west of the Mississippi: history, general examination, abdominal and external genital exam, urinalysis including a stained smear, prostate exam, plain x-ray, phenolsulfonephthalein test (PSP), and residual urine. [Bloom DA, Hinman F Jr. Frank Hinman, Sr: a first generation urologist. Urology. 61:876-881, 2003.] Color and other sensory inspection still matter and while details have changed, urology is diminished somewhat when its practitioners no longer personally inspect urine grossly and microscopically, favoring instead automated readout from machine or lab.
Five.
The story of urology at the University of Michigan was last told 20 years ago just after the Urology Section in the Medical School Department of Surgery emerged as a full-fledged department alongside its sibling disciplines of Neurosurgery and Orthopaedic Surgery. Much happened in the next 20 years to justify a new rendition of the story and additionally much more has been learned about the earlier years. The new book should coincide with the Michigan Urology Centennial, beginning later this year. Urology is a microcosm of modern specialized health care, but its roots are also of particular interest as the first designated medical specialty in Hippocratic times and the stories since then of the discoverers, progression of skills, and innovations that led to 19th century genitourinary practice and 20th century urology should be retold and interpreted for each new generation.
No story is ever complete, in its recollections of the past, because only partial relevant knowledge is known to any author and myriad other details of the cultural and physical soups surrounding those facts are mostly lost to historical recollection. Lucky historians may find, reconstruct, resuscitate, or recover useful details, but all stories are largely narratives of imagination and facts, whether true facts or otherwise, in the words of the late urological scientist, Don Coffey. Stories, even as particular as one of an academic urology unit, are enriched by the context of its people, events, and circumstances. For example, it’s inconceivable to consider urology at Michigan without understanding Moses Gunn, and any appreciation of Gunn requires the context of the Civil War. In that sense, the Michigan urology story aims to be rich in context.
Six.
The bicentennial edition of Howard Peckham’s sesquicentennial work, The Making of the University of Michigan, by Margaret and Nicholas Steneck is indispensable to understanding this institution. The Stenecks proposed, metaphorically, that this university began with a single strand that represented the foundational aim of the university to disseminate knowledge and embracing education at all levels. This strand thickened over time and became joined by a second strand, turning around the first one, the new strand representing knowledge itself, that must be interpreted, renewed, created, and disseminated through explorations, criticism, research, and invention. The Stenecks identified yet another part of the braid.
“Now there is a third strand wound with the other two. The University touches more than just its young students and faculty. It gives services to the State that help maintain it; it aids citizens who never enroll. These services began when its hospitals received perplexing cases from all over the State. It continued with the upgrading of high schools, the testing of municipal water supplies, with experiments in reforestation, testing programs for state highways. It supplied reading lists for club programs, lecture series for enlightenment, and musical concerts for entertainment. It expanded to research contracts for Michigan industries, development of new products for manufacture in Michigan, seminars for business executives, realtors and assessors, state college presidents, and refresher demonstrations for physicians and dentists. It provided radio and TV educational programs for all. Teaching–research-and service. These are the warp and woof of the University today.” [Peckham HH. The Making of the University of Michigan. 1817-1992. Edited and updated by ML Steneck and NH Steneck. University of Michigan. Ann Arbor. 1967, 1994. p. 1-2.]
A better term for “service thread” is that of public goods, and today those public goods extend far beyond the state of Michigan to the world at large. Universities, since the Middle Ages, have been the single entity in human society to attend consistently and dutifully, albeit imperfectly, to the human and planetary future. In the past few centuries the university, or the Academy as some call it, has extended from small Ivory Towers that educate a particular narrow subset of learners, to complex Multiversities with broader aims such as the Stenecks listed.
Seven.
Mission homeostasis. The University of Michigan entered the 20th century with a more complex, but clearer iteration of an academic medical center than it displayed at its start when medical education was the sole basis for its existence. The Chemical Laboratory in 1856 introduced the service of chemical analysis to medical education, clinical practice, and scientific discovery. A more complete linkage of medical education to clinical practice came with Michigan’s first university hospital in 1869 and by its third iteration in 1891 the triple mission of an academic medical center was fully in place, although confusion over priorities played out in such disputes as moving the medical school closer to large urban populations and hospitals, compensation of clinical faculty, and criteria for academic promotion.
Mission balance continued to confuse faculty and perplex leadership for that next century and into the present one. History brings some clarity to the matter: the University of Michigan Medical School began with an educational mission of training the next generation of physicians, research followed quickly initially to refine biochemistry in the service of the public, and clinical care was recognized as the necessary milieu for medical education and research. Among these three parts of the conjoined mission, clinical care is the moral epicenter, trumping any other part of the mission at any moment. Furthermore clinical care, a matter of complex intellectual teams, is the financial engine that currently underpins the other missions. Any great academic medical center must be first and foremost a state-of-the-art health care system that not only delivers excellent patient-centric service, but also studies and improves its systems of care and technologies along with its many scholarly and clinical disciplines. Clinical teams are the essential center and most important deliverable of academic medical centers. [Above: scribe’s heart measured against “feather of truth.” Book of the Dead, c. 1,265 BC. National Geographic, Ancient Egyptians. May 2009.]
Eight.
No Property in Man. January 15, 1929, the birthday of Martin Luther King, Jr., is celebrated later this month for his role in the slow, halting, and sometimes retreating movement towards universal human rights, a struggle that remains a very incomplete paradigm shift worldwide. [Above: MLK 1964.] Extending Mahatma Gandhi’s methodology of nonviolence and civil disobedience, King fought inequality through resistance that was nonviolent on his side of the bridge to change laws, public sensibility, and hearts and minds. Martin Luther King Day is celebrated around the time of Dr. King’s birthday, January 15, but the specific day this year will be January 21 according to the Uniform Monday Holiday Act. Michigan Representative John Conyers along with US Senator Edward Brook (MA) offered the first bill in Congress to honor King, but it fell short of passage by a few votes in 1979. In 1983, President Reagan signed the final bill to establish the day of remembrance, which commenced in 1986, also establishing a federal commission to oversee observance of the holiday. In 1989 President George HW Bush made Coretta Scott King a lifetime member of the commission. Toronto, Canada, Hiroshima, Japan, and Wassenaar, Netherlands also honor Dr. King with public observances.
We don’t close clinics, operating rooms, or phone lines for that day at Michigan (that would hardly have been in the spirit of Dr. King, anyway), but the occasion offers a time for reflection, study, relevant academic talks, and renewed efforts toward the unfulfilled paradigm shift to universal human rights. A good friend and Americana scholar, Jim Beuche, recommended a book called No Property in Man, by Sean Wilentz. In the spirit of this month, this is a “must-read” for 2019. Wilentz explains the issue starting at the Federal Convention (U.S. “Constitutional Convention”) in 1787.
“Descriptions of the Constitution as proslavery have misconstrued critical debates inside the convention. They have slighted the anti-slavery impulses generated by the American Revolution, to which the delegates, for better or for worse, paid heed. They have missed the crucial subtlety, which is this: although the framers agreed to compromises over slavery that blunted antislavery hopes and augmented the slaveholders’ power, they also deliberately excluded any validation of property in man.” [Wilentz. No Property in Man. Harvard University Press, 2018.]
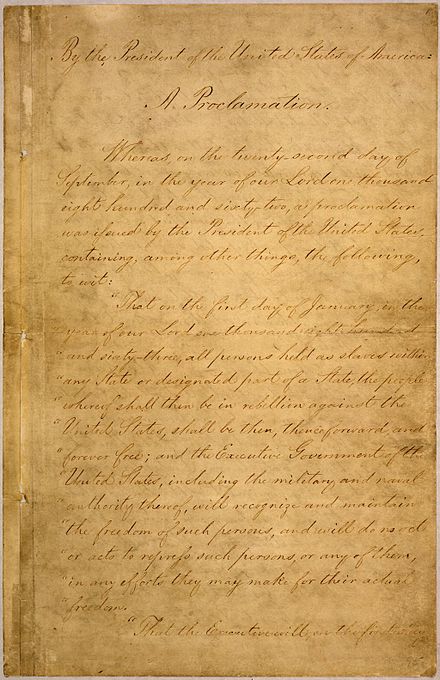
Many forces assembled to abolish slavery in America, but Wilentz argues that the United States Constitution, the Republican Party (“an antislavery mass organization unprecedented in world history”), Proclamation 95 (Lincoln’s Emancipation Proclamation), and the 13th Amendment, legally abolished any legitimacy of the notion of “property in man” in America. [Below: page one of the five-page Emancipation Proclamation. National Archives.]
At President Kennedy’s suggestion, King led an effort to draft a Second Emancipation Proclamation, that would have outlawed segregation and expanded equality, but Kennedy’s Executive Order 11063 fell short of the draft. Lyndon Johnson’s Civil Rights Act of 1964, fulfilled more of King’s aspiration. That year King won the Nobel Peace Prize at age 35. He was assassinated in 1968 at age 39.
Nine.
Harvey Ball (1921-2001) designed the Happy Face to repair a decline in morale after the bumpy merger of two insurance companies. How effective the ideogram was in that instance is not clear, but Ball earned $45 for it and never applied for trademark or copyright. He never voiced regret for giving his symbol to the public, even after it became a universal symbol. Ball was born and raised in Worcester, Massachusetts, served in the Pacific Theater of WWII with a Bronze Star for heroism at Okinawa, started his own advertising company in his home town in 1959. One day, in 1963, he drew Smiley.
As a matter of law, copyright goes back to 1709 and the Statute of Queen Anne of Britain, the last monarch of the House of Stuart and the same Anne portrayed in the current film, The Favourite. Another current film, Mary Queen of Scots, portrays the start of the House of Stuart two centuries earlier, with the conception and birth of James, later first Stuart and first king to preside over England and Scotland.
The U.S. Constitution in 1787 includes a Copyright Clause (Article 1, Section 8), recently updated with the Copyright Act of 1976 and the Sonny Bono Copyright Term Extension Act of 1998, also called the “Mickey Mouse Protection Act” [Above: Queen Anne’s Statute. Below: Bell’s graph of US Copyright law expansion. “©1999-2008 Tom W. Bell. All rights reserved. Fully attributed noncommercial use of this document permitted if accompanied by this paragraph.” Wikipedia.]

Three days ago (Jan 1, 2019), according to U.S. copyright laws, all works published in 1923 entered the public domain. Sonny’s name was likely linked more to his music than his love of 1923 literature. (Wikipedia.) Works published then were to have entered the public domain in 1999, but were granted postponement by 20 years when Congress extended their copyright length with the Bono Act. Willa Cather’s A Lost Lady, Agatha Christie’s The Murder of the Links, Joseph Conrad’s, The Rover, Kahlil Gibran’s The Prophet, Marcel Proust’s The Prisoner (vol. 5 of In Search of Lost Time), William Carlos Williams’s The Great American Novel, and Virginia Wolfe’s Mrs. Dalloway in Bond Street were so reprieved.

[Above: copyright applied. Below: public domain.]

Ten.
Matula Thoughts analytics, 2018. We have no sense of the readership of the monthly What’s New delivered by email, but the web version, MatulaThoughts.org had 3454 views last year compared 3173 views in 2017. Viewers came from 89 countries, ranging from a few viewers in 35 countries, to 54 in Germany, 70 in the U.K., 87 in Canada, and 2578 in the US. Most views are cursory, but we enjoy hearing back directly from periodic careful readers who challenge our facts and alert us to errors.
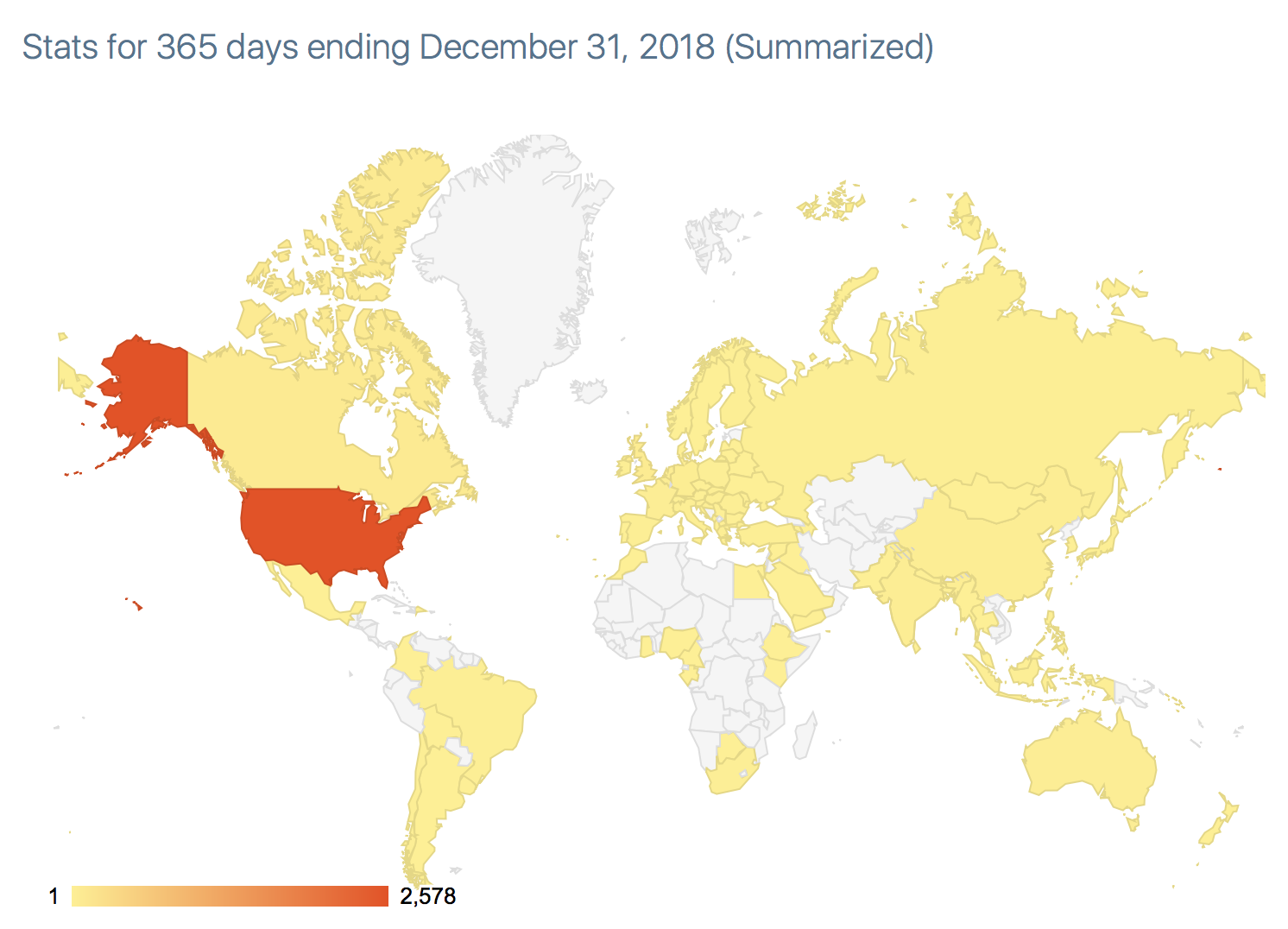
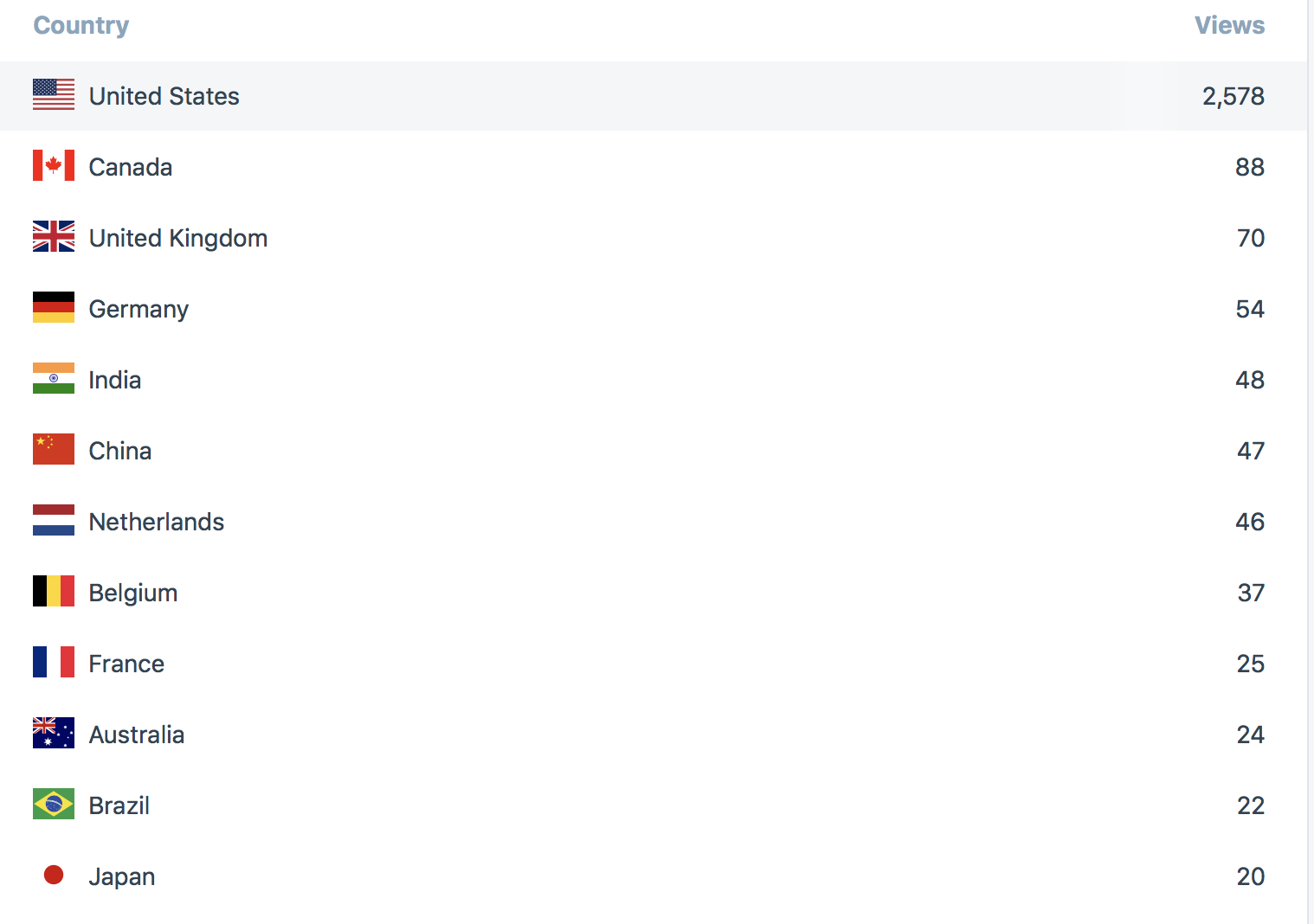
[Above: analytics 2018.]
New Year 2019 began on a Tuesday and a short work week ends today for most people, but health care is a 24/7 business and by necessity we will offer more scheduled afterhours and weekend services at Michigan Medicine Urology, even though we have been doing so formally and informally for years. It is curious that most calendars begin each week on Sunday, although for most people that day is the end of the week and weekend, with the next week beginning at sunrise on Monday.

The 1902 fantasy film, Le Voyage dans la Lune, by Georges Méliés, shows an oversize spacecraft planted in the right lunar eye. We don’t have to travel 240,000 miles to stick it to a heavenly body, because Homo sapiens is doing this well enough right here at home on Earth, but possibly 2019 will be a turning point for planetary stewardship.

[Above: Schedel’s World History or Nuremburg Chronicle, 1493. Below: Earthrise, December 24, 1968. Apollo 8 astronaut William Anders.]
©David A. Bloom 🙂
University of Michigan, Department of Urology, Ann Arbor