
![]()
Challenges of FY 14, leadership, conflicts, & our successors.
1. Not so long ago fiscal year 2014 loomed large as an ominous transition point in health care with the collision of multiple forces of major impact. The rising rate of spending relative to GDP, the struggling world economy, climate change, expensive new pharmaco-technology, increasing economic and healthcare disparities, aging populations, the growing complexity of the health care work force, unintended consequences of large scale legislative health care legislation, underfunded necessities of research and education, duty hour dysregulation, are only some of the many forces that quickly come to mind. Other factors are less immediately obvious, but no less significant. New appreciation of the complexities of chronic disease management has rendered our models of health care delivery archiac (e.g. the primary care-specialty care model, employer based coverage, and even the very idea of “an insurance model” to manage health care for a large population). The effects of gerrymandering in determining election outcome, and hence legislation and public policy, similarly have impaired the public good. All of these things have come together now, more than ever before, to destabilize the economy and structure of healthcare in the United States.
2. Nevertheless, this feared watershed fiscal year is in it’s final month and, for the most part, the essential transactions of health care delivery – clinic visits, medication prescription, diagnostic testing, operative procedures, provision of supplies, education, research, and innovation are still happening on a daily basis even though this work seems to be done against the grain with increasing difficulty. We will soon have our FY 14 numbers (patient visits, operative procedures, RVUs, grant dollars, satisfaction scores, papers written, patents claimed, operational margins, days of cash on hand, etc.) and analysis of these will show us where we stand. However it comes out, even if our fiscal head is above water which we expect, we will be standing well below our potential as a department, as a medical school, as a health system, as a university, as a state, and as a nation. Irrespective of the constraints of the larger environment (including our self-inflicted wounds of the HITECH Act, legislative gridlock, and reactive regulation such as the duty hours story) we have the ability and duty to our patients, trainees, employees, community, and our children to do our work better. While the FY 14 boogeyman didn’t bring the world to a screeching halt, we still need to rapidly find new ways to maintain the missions of academic medicine – clinical care, education, and research. Underpinning all this is our essential deliverable: kind and excellent patient-centered care, thoroughly integrated with education and innovation at all levels. If we get this right, one patient at a time as well as one system at a time, then most everything else we want will follow.
3. Today’s date, June 6, is a big anniversary for a far more monumental watershed point in time for mankind. Operation Overlord was launched on this day in 1944. Had this massive organizational feat failed the world would be very different today. In fact it’s leader, Dwight David Eisenhower, was not so sure of success given the myriad contingencies in play beginning at the launch of Overlord exactly 70 years ago and he accordingly prepared an alternative brief statement on July 5 to be released in case of failure: “Our landings in the Cherbourg-Havre area have failed to gain a satisfactory foothold and I have withdrawn the troops. My decision to attack at this time and place was based on the best information available. The troops, the air and the Navy did all that Bravery and devotion to duty could do. If any blame or fault attaches to the attempt it is mine alone.” Eisenhower offered no optics, spin, or scapegoats.
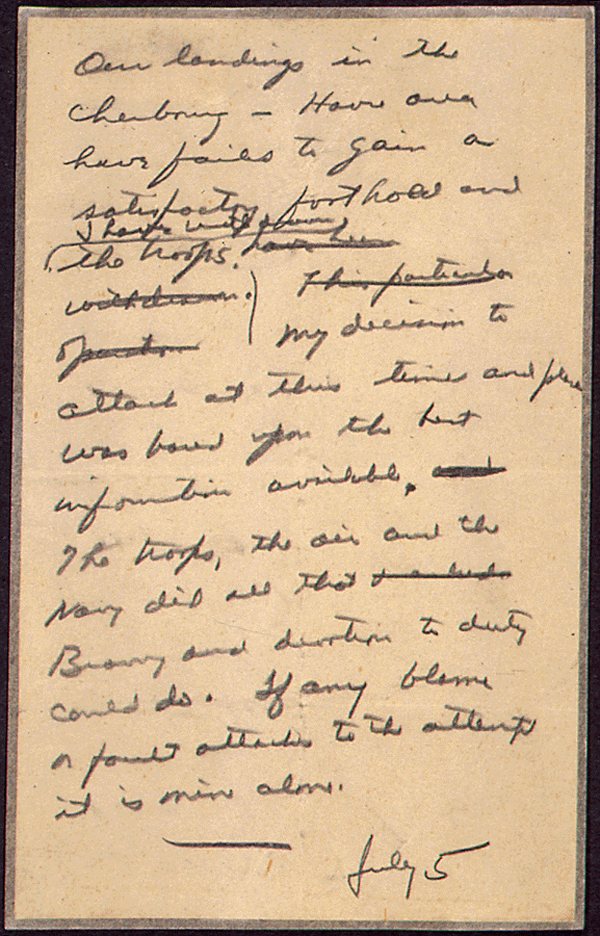
[The Eisenhower mea culpa never needed to be sent.]
4. Eisenhower was not unchallenged as a leader or soldier even though he had the trust of Roosevelt and Churchill. His British counterparts were demeaning: Bernard Montgomery said “Nice chap, no soldier” and Alan Brooke proclaimed that Eisenhower knew nothing about strategy and was “quite unsuited” to be Supreme Commander. In retrospect, those comments seem to reflect mere petty jealousies as the outcomes of Eisenhower’s leadership at that key point in time dwarf any accomplishments of those detractors. Leadership matters greatly. While leaders have great latitude in times of relative peace and stability, they have consequential impact when times get tough. The world today would most likely be very different had it not been for Eisenhower, Roosevelt, and Churchill seventy years ago, and the same holds true as such for Lincoln and Washington in their times as well. Much more recently and locally look at Bill Ford and Alan Mulally for extraordinary leadership success. On the other end of the spectrum leaders of very different character such as Pol Pot and Adolph Hitler hijacked their constituencies and neighbors into terribly dark days. This is evidence of the problematic duality of our species. We are the only one of the rare eusocial species who can deliberately select leaders and determine our governance – but that is another story, better told by E.O. Wilson. [Two books of reference: a.) Anthony Beevor. D-Day. The Battle for Normandy. b.) Edward O. Wilson. The Social Conquest of Earth.] [Pictures – Normandy beach 70 years ago and same beach and American Cemetery on my visit in 2010]



5. Leadership was at play last month at the AUA national meeting in Orlando, on many podiums and in many committee sessions. One noteworthy example was the Michigan Urological Surgery Quality Collaborative (MUSIC) conceived by Jim Montie and “Eisenhowered” by David Miller. At the MUSIC session I saw urological colleagues participating from around the state including a number of our own former students and residents. Dr. Miller and Dr. Brian Stork gave excellent presentations, highlighting the beautiful social/scientific collaboration of urologists who have, through trust and hard work, pooled their individual and local experiences to figure out to deliver better care at better value in collaboration with Blue Cross/Blue Shield. This should be a model for the future in health care. Especially inspiring was to see how MUSIC has brought private practitioners to podium presentations and to authorship positions thus erasing the “barrier” between the academic and non-academic sides of urology. Leadership has also been in play with Stuart Wolf’s amazing work overseeing the AUA guidelines. Prominently visible was the running video on guidelines showing Michigan faces throughout the AUA including Stuart, Quentin Clemens, and Ann Gormley. John Park’s Mott video was also running outside the pediatric sessions, showing Julian Wan, Vesna Ivancic, and Kate Kraft as well as John Park and Carla Garwood, representing our pediatric nursing team. A video also showed members of the prostate SPORE group. The Reed Nesbit Society held its reception on Sunday night. This has become a lovely annual habit and is financed by both the Department of Urology and the Nesbit Society. This year we hosted around 120 people. Friends of the department, new and old alumni, faculty, and residents acquaint or re-acquaint themselves. If you missed it this year consider joining us in 2015 in New Orleans on Sunday, May 17. Perhaps the biggest news of the meeting was the awarding of the AUA Gold Cystoscope to our Associate Professor Will Roberts later in the convention. Ed McGuire received this honor back in 1982, so out of a total of 38 Gold Cystoscopes, Michigan Urology now accounts for two. David Miller was awarded the Society of Urologic Oncology (SUO) Young Investigator Award. Ted Skolarus, Jeff Montgomery, Florian Schroeck, and Khurshid Ghani were awarded Best Abstract at the 2014 VA Forum. Bahaa Malaeb, Aruna Sarma, and Rod Dunn received Best Poster Award for their work on the relationship between diabetes and sexual dysfunction.

[Photo by Wendy Roberts]
6. National meetings of specialties are the fundamental marketplaces for the ideas, products, and talents of healthcare processions. Large organizations such the AUA, ACS, ASCO, AAP, EAU, or SUO may seem like an alphabet soup to outsiders, but they are the interfaces between today and tomorrow for medical specialties. Each year in between the meetings faculty, residents, and research teams develop ideas, create hypotheses, test products, and perform other acts of scholarship even while doing the never-ending daily work of clinical care and education of our successors. The chance to stand at a podium and present one’s observations to the world of urology at large is a big moment for residents, and aggregation of those moments develops reputations and careers for faculty. Michigan Urology had a big year at Orlando’s AUA meeting. We used to try to count the number of appearances for our faculty, residents, and students at this meeting and found the count running well beyond 100, but this year I won’t even try that little exercise of hubris. The bottom line is that Michigan Urology’s people and ideas are a major force in this marketplace of urology. I had too much fun talking and taking pictures at our Nesbit reception so I deferred my brief “State of the Department” presentation for an appendix in this “What’s New.”
7. The AUA national meeting is heavily subsidized by urologists as well as the corporate world. We and our departments spend big dollars on the research that produces the talks. We also pay travel expenses for the faculty, residents, and nurses who give the talks and listen to others. The practice of urology is a profession that exists within the social industry of healthcare. We depend upon social opportunities such as this annual meeting to exchange and stimulate new ideas, to see new products, to network for new opportunities, to find jobs for our trainees, and to develop collaborations. While replete with opportunities, the interfaces of the medical profession, industry, and academia have ethical risks. We are all human, and some of us test boundaries of self-serving behavior more than most others. A smaller number, reflecting the dark side of our duality, wander into territories of mischief or even deliberate wrongdoing thus rules are necessary. We recoiled when we read about the Ivy League professor promoting his (unacknowledged) proprietary antihypertensive drug to a class of medical students as THE drug of choice, or learn of an orthopedic surgeon routinely using his own invention in patients without full disclosure of his commercial interest. Our own institution is not blameless as seen recently by the professor in another department who gave confidential drug trial results to hedge fund operators that allowed insider trading. These people are scoundrels and dirty our profession. Not all conflicts are purely monetary and some are conflicts of commitment. It is not uncommon for many of us to try to wear too many hats, even though our heads are only finite in dimension. In fact we each actually do need a few hats, for rain, cold, construction work, mosquito protection, etc. Ego, however, makes us overestimate our head size tempting us to accept a few too many. You could call this phenomenon the hat trick of ego or perhaps “the blinding effect of arrogance”, a risk for each of us.
8. Academia and industry need to intersect for the public good. We sometimes manage this intersection well and other times not so well. One good example is histotripsy, a technology invented here at Michigan by a team including our own Will Roberts, along with radiology and biomedical engineering colleagues. As a department, Michigan Urology has invested a decade of time and money in Will and this idea. Ultimate product development, however, exceeded our capacity and required initial venture capital to the tune of $11 million. Within only about four years now clinical trials for BPH are underway (with full disclosure) at a number of sites – Tim Schuster in Toledo (Nesbit 2004) did the first histotripsy prostate enucleations. We have a thorough conflict management plan that details the extent of our departmental involvement in this product development and its trials. We are doing this well and properly. It is important to develop good standards to manage conflicts of interest and conflicts of commitment, although ultimately we must depend on shared values and appropriate behaviors. [Actually, and somewhat unfairly, the University of Michigan through its policies rather than our Department of Urology, will assume most of any financial gain if HistoSonics Corporation is successful.]
9. Although I was present at the discussions and votes around our medical school’s new conflict of interest policy, I was uneasy supporting the stipulation that faculty, residents, and nurses must refuse hosted social occasions at national meetings. As we prepared to go to the AUA meeting messages went out that our new conflict of interest policy warned against accepting food or drinks from the pharmaceutical and industrial representatives who otherwise would be with us in Orlando supporting the meeting. In the past I have freely enjoyed the hospitality of, for example, the Olympus Corporation with our representative Bill Herpek while on other occasions I’ve picked up the check for the burgers he and I had at the concession stands in the exhibit halls. Bill has become a friend and colleague for 25 years, quickly available for replacement scopes in the OR when urgent repairs are necessary, or finding us good deals (in the world of competitive bidding) when we need new technology. The extent of our mutual hosting has really been nickel and dime, not paid excursions, serious gifts, or stock options. (In full disclosure he did give me a wildlife calendar once.) Might someone assume that our friendship or the burger I bought him translated into a sweeter deal for the cystoscopes we purchased? Doubtful – but our relationship does provide a basis for fair deals and open communication. It’s not just our own Michigan policies that don’t seem quite right. When we had Marston Linehan here recently for a Von Hippel Lindau symposium, NIH policy required him to pay for his own dinner at the event. Given the shenanigans of Congressional and other leaders, I am embarrassed by the double standards. Our colleague here at the University of Michigan Charles Eisendrath tells us that in his journalism career the self-imposed standard was that “if you can’t eat it or drink it, you shouldn’t take it.” On the other hand the egregious exploits related to insider trading I mentioned earlier involved far more than cheeseburgers, but I’d contend they didn’t begin on the ”slippery slope of a lunch” at a national meeting, but rather involved cozy self-serving deceit right from the start. How about participation on heavyweight national boards by university leaders? I have heard the many “pros” of the argument, but really our top academic and health system jobs are not only quite well compensated but they also seem to be demanding enough on a 24/7 basis. Yes the interface between academia and industry needs to be somewhat fluid, and yes leaders “can learn things” and develop relationships on major boards. On the other hand, proper board service is demanding of time and commitment, things that might be more reasonably offered when individuals are no longer in the pilot’s seat for a major enterprise. The hat trick of expertise is an alluring illusion and we are each susceptible to its temptations. No policies or laws can substitute for a good internal compass, although any compass can be swayed by strong elemental forces (iron, silver, or gold). An essential part of our jobs as teachers and role models in the health care industry is the duty of imparting a strong moral compass to our successors. As I look at our Nesbit alumni – it seems that Michigan Urology has done this well for nearly 100 years.
10. Our foundational mission at the University of Michigan Medical School and Department of Urology is to train our successors, and the evidence of our success is beautifully visible each year at the Nesbit AUA Reception. As you know, the context for education of our successors is necessarily the practice of medicine amidst the innovation of the science, technology, and systems of healthcare. Our essential deliverable of all this is kind and excellent patient-centered care, thoroughly integrated with innovation and education at all levels. The basic building blocks of education are medical school and residency training. Michigan’s medical school graduation took place just a few weeks ago and our 169 graduates will go out to start their residencies in the next few weeks. Michigan students are highly prized in training programs around the country, reflecting the excellence of our medical school and the departments in which students discover their careers. The match rate this year was 100%, meaning that all Michigan students were accepted by the training programs they sought. Of these 28% will stay at Michigan for training and 32% will remain in our state. The others will go to top programs around the country.
Five Michigan medical students went into Urology this year: Denise Asafu-Adjei to Columbia University Physicians & Surgeons in New York, NY; Spencer Hiller to Beaumont Health System in Royal Oak, MI; Zachary Koloff to University of Michigan in Ann Arbor, MI; Kola Olugbade to SUNY Downstate Medical School in Brooklyn, NY; and Brian Orr to Indiana University Medical Center in Indianapolis, IN.
Of our four new urology interns coming to our program: Ella Doerge from Baylor College of Medicine in Houston, TX; Zachary Koloff from University of Michigan Medical School in Ann Arbor, MI; Ted Lee from New York University School of Medicine in New York, NY; and Parth Shah from University of Texas Medical School at Houston, TX. Michigan residencies pick the strongest students from other schools as well as ours – of the interns that entered in 2013 for all specialties here 41% were members of AOA, the medical school honorary society.
We have three new fellows: Sapan Ambani from University of Michigan for a two-year endourology fellowship, Lindsey Herrel from Emory University for a three-year urologic oncology fellowship, and Yahir Santiago-Lastra from Massachusetts General Hospital in Boston as a clinical program trainee in the female medicine and reconstructive surgery (urology) for two-years.
Graduating Chief Residents: Sapan Ambani will be staying with us for an endourology fellowship. Dan Miller will be doing a fellowship in endourology and minimally invasive surgery at the University of California San Diego/Kaiser Permanente. Jackie Milose is going to Northwestern in Chicago for a GURS Fellowship. Matt Smith is headed to Muskegon to work with the team of urologists at West Shore Urology. Fellows: Nina Casanova is completing her pediatric urology fellowship. Florian Schroeck is joining the faculty as an Assistant Professor in the Department of Urology at Geisel School of Medicine at Dartmouth. Anne Suskind is headed to UCSF on the faculty as an Assistant Professor in the Department of Urology.
The highest step in the academic ladder is the rank of Professor and this title was granted by the University to Quentin Clemens, Khaled Hafez, Brent Hollenbeck, and John Park. Jeff Montgomery became an Associate Professor. Academic promotions are recommended and approved by each departmental promotion and appointment committee, then by one of the three Dean’s Advisory Committees (the faculty vote on memberships for these), then by the Medical School Executive Committee (also elected by faculty vote), then by the Provost, and finally by the Regents. These promotions are effective September 1.
Best wishes, and thanks for spending time on “Matula Thoughts.”
David A. Bloom, M.D.







