WN/MT September 4, 2020
Truths & mousetraps.
2450 words
One.

This September feels different. It’s no longer just a matter of seasonal daylight contraction, but also a fact of social shrinkage and much more. Summer 2020 was unlike any before and academics this autumn, from pre-school through medical school, will also be totally different. Innovation is in demand to navigate the crises in business, education, medical practice, public policy, sports, and much of everything else in daily life. The good news is that humans are good at creating new and better mousetraps, although not so good at escaping the mental mousetraps of their own follies. [Above: September ground litter, Scio Township 2018.]

Hunkering down in the first weeks of this 2020 Covid pandemic, I reread Howard Markel’s book, When Germs Travel: Six Major Epidemics That Have Invaded America and the Fears They Have Unleashed. Written in 2004 it holds up very well now, 16 years later, offering pandemic perspective. Howard, shown above, has frequent pieces on Public Broadcasting Service (PBS), maintains the 1918 Influenza Epidemic Encyclopedia in a UM Digital Archive (chm.med.umich.edu), has a recent Medical Dispatch in the on-line New Yorker Newsletter (August 6, 2020), and a new book on genetics, called Helix, in the works.
Lessons learned from past infectious disasters tend to be forgotten. Face-masks, hygienic measures, social distancing, and validated vaccines unquestionably mitigate transmission and acquisition of germs – medical scientists and the informed public know this much is true, but why doesn’t everyone else?
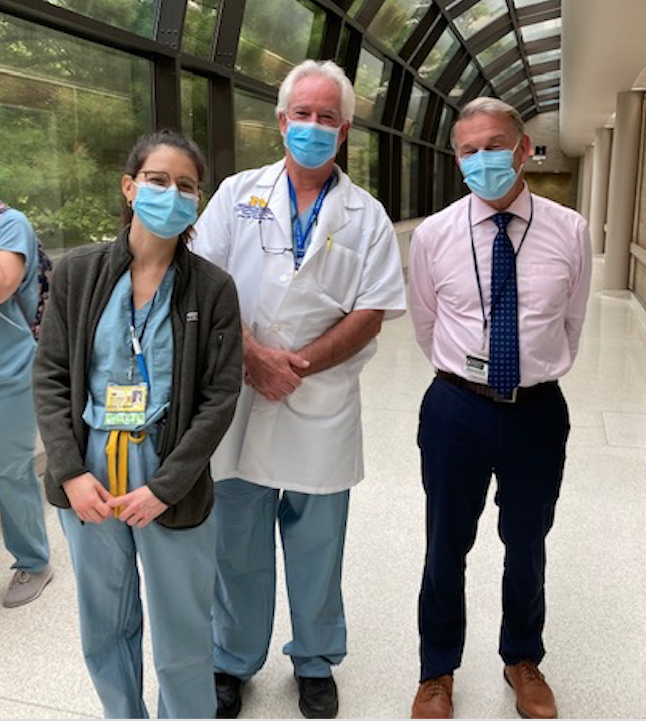
Weaponization of those protections, particularly the ridiculously easy solutions of face masks and social distancing, as political gestures is sadly bizarre. Whether it’s a matter of ludditism, partisan ideology, or mere ignorance will be sorted out by future social critics. As a person who wore face masks in operating rooms for nearly 50 years – alongside uncounted colleagues, nurses, and scrub techs – the claims of “medical reasons” why some people “can’t wear a mask” are incredulous – as unconvincing as claims of pet snakes or birds as “medically-necessary” travel companions on airplanes. The parallel contention that the duty to wear masks violates personal freedom is certainly a far cry from anything reasonably derived from common sense or the American Constitution. It’s not surprising that similar skirmishes sprung up with the Great Influenza epidemic in 1918, when education and science had not quite universally settled the germ theory in minds, but it is astonishing to find such shenanigans a full century later. [Below: mask-wearers at University Hospitals, senior medical student Annie Minns and professors Cosmas Van De Ven and David Spahlinger – social distancing briefly waived for the photo op, Aug. 2020.]
Two.
Basic truths. Mousetraps for infectious diseases have come and gone, but routine hygiene and simple impediments to germ transmission (face masks & distancing) seem to be basic truths.
Historical medical relics were facts once true for their times. The iron lung for the respiratory failure of polio was a “better mousetrap” in the 1930s through the 1950s. The original iron lung used two vacuum cleaners to change pressure in an iron chamber, compressing and inflating chests and lungs of children lying within them. Philip Drinker (1894-1972), teacher of industrial illumination and ventilation at Harvard Medical School (alongside famed UMMS graduate Alice Hamilton), came up with a popular design, the “Drinker Lung.” Haven Emerson (1906-1997), son of NYC Health Commissioner, improved the device by placing the patient in a bellows within the chamber. Emerson’s Iron Lung was quieter, lighter and only $1,000, half the price of others. It remained in production until 1970, when polio largely had disappeared from much of the planet due to vaccination. Coincidentally this is a good opportunity to refer to Markel again. [H. Markel. “The genesis of the iron lung,” Arch Pediatr Adolesc Med, 1994; 148 (11): 1174-1180.]
Polio outbreaks were dreaded in the summer. As a child, I noticed post-polio limps in many people and heard about iron lungs, seemingly ubiquitous in every hospital. The July newsletter, Matula Thoughts, referred to our friend and colleague Skip Campbell who was hospitalized at “old” University Hospital as a youngster to treat his polio. That was just around the time polio began to disappear when field trails of Salk’s vaccine, directed from UM by Thomas Francis, proved it “safe, effective, and potent” in 1955. The Sabin vaccine soon proved better. Oddly, U.S. authorities supported only the Salk clinical trial, and Sabin had to prove his vaccine in field trials in the Soviet Union. This was no small feat in the political theater and Cold War of the 1950s, but Sabin, against the grain, organized the trials and the world ran to his better vaccine. Even now, however, global polio eradication is incomplete. [L. Roberts, Science, 367:14, 2020.]
Situational necessity, inspiration, and competition fuel better medical mousetraps, but innovations happen best in open societies. Iron lungs were useful in their times but gave way to better innovations. Modern respiratory physiology knowledge and more sophisticated ventilatory technology sprang from other responses to polio. [J. West. “The physiological challenges of the 1952 Copenhagen poliomyelitis epidemic and a renaissance in clinical respiratory physiology,” J. Appl Physiol (2005); 99:424-432.] So once again, let’s celebrate democracy and free speech: innovation -with its validation, dissemination, and improvement – thrive best in the fertile social soil of personal freedom and open expression.
Three.

Mousetraps. “If you build a better mousetrap the world will beat a path to your door.” Such is the power of “the market” at large, whether the market is commercial or intellectual. Flat Earth maps may lead some mousetrap-seekers astray, but most people find their ways to better ideas and technologies. [Above: Conventional Victor Mousetraps at Barnes Ace Hardware two for $1.69 vs. Intruder’s Better Mousetrap two for $5.99.]
Ralph Waldo Emerson (above), the source of the phrase, actually wrote:
“If a man has good corn or wood, or boards, or pigs, to sell, or can make better chairs or knives, crucibles or church organs, than anybody else, you will find a broad hard-beaten road to his house though it be in the woods.”
Emerson knew something about paths in woods, not only living among them, but also hiring Henry David Thoreau as his property caretaker when the journalist of Walden Pond needed a paying job. A future tenuous connection between Emerson and Ann Arbor materialized after James Elliott Cabot (below), Emerson’s friend, executor, and biographer, fathered Hugh Cabot, who instigated the first century of Michigan Urology in 1919. “Elliott” Cabot (1821-1903, shown below), as he was known, was a brother of Dr. Samuel Cabot III and shares facial physiognomy with at least three of his sons: Michigan’s first urologist Hugh Cabot, twin brother Philip, and internist brother Richard Clark Cabot.
Four.
Medicine has had its share of mousetraps. Enduring diagnostic tools from antiquity – the medical history, physical examination, rudimentary vital signs, and uroscopy (body fluid observation) – have been tested and refined in medical marketplaces over millennia. For urine inspection, pottery gave way to glass matulas, microscopes extended visual inspection into the microscopic world, chemical analysis opened up molecular composition of urine, and bacteriology led to identification of pathogens. Innovation similarly propelled stethoscopes (1816), x-rays (1896), electrocardiograms (1920s), CAT scans (1970s), and MRIs (in wide use after 2000) into the clinical marketplace. The technology of modern urology is too rich a topic for further mention here, except to take note of Nesbit’s transurethral resection of the prostate, Lapides’s clean intermittent catheterization, and McGuire’s leak point pressure.
Amidst high-tech mousetraps of today, the simple face mask used in ORs around the world is clearly effective against dust and infectious droplets (liquid dust). A recent JAMA article by Brooks, Butler, and Redfield, suggests we implement universal masking for all healthcare workers and patients in clinical situations, affording both personal protection and source control. Aerosol particles range from sub micrometers (0.0001) to a full ten micrometers (microns) in diameter. By the way, 1000 microns equals 1 millimeter. Even simple cloth face coverings substantially limit forward dispersion of exhaled respirations in the 1-10 microgram range. [JAMA 324:635, 2020.] [Above: ORs & face masks in Mainz, Germany. Below: airborne particles, source – Wikipedia, Particles. Horizontal axis in micrometers, or microns.]
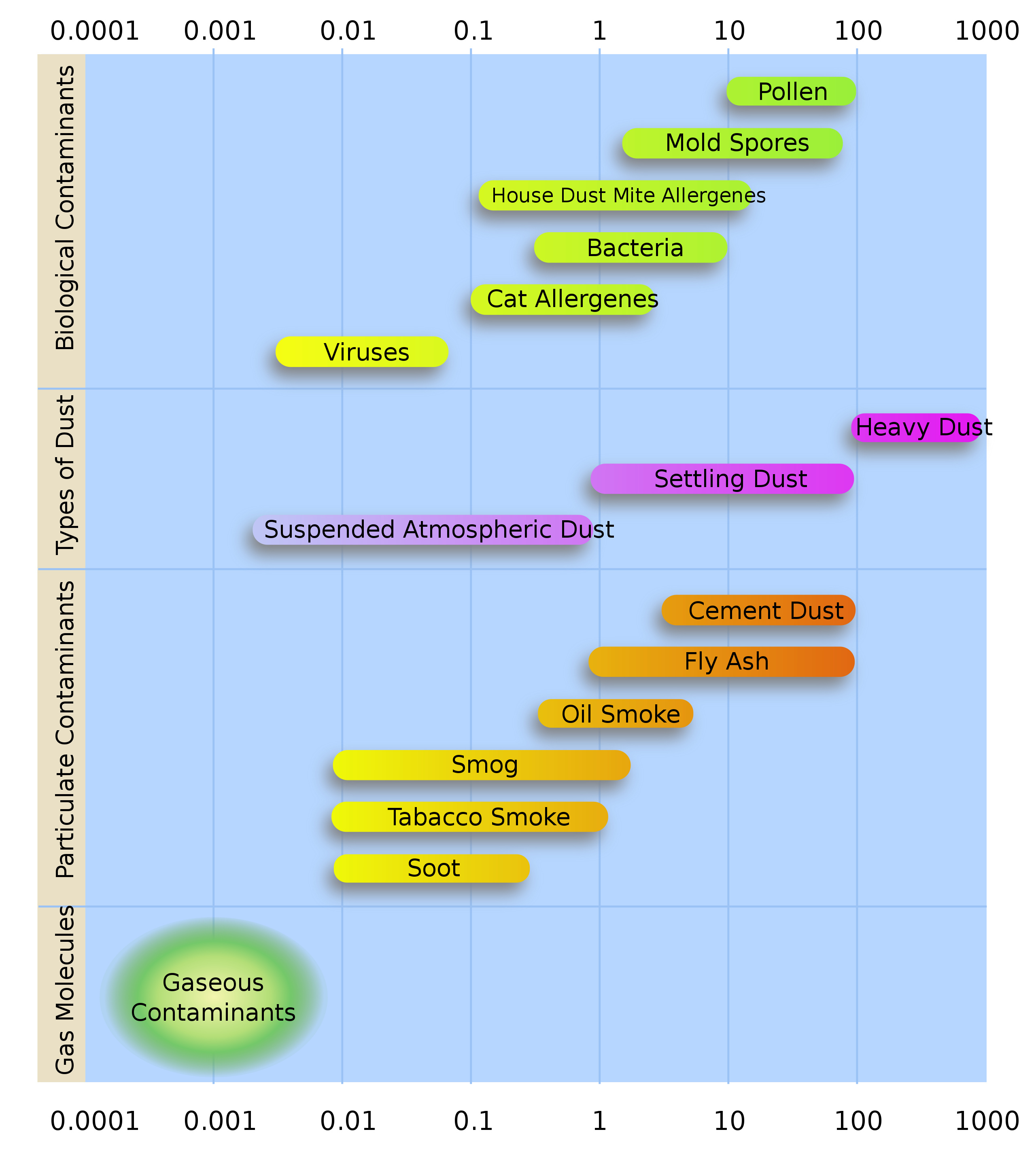
A higher level of filtration than routine face masks, the N95 mask, was designed to meet the U.S. National Institute for Occupational Safety and Health (NIOSH) specification of filtering at least 95% of airborne particles. To be fully effective, it requires “fit-testing,” an annual ritual at Michigan Medicine along with the TB testing, that few knew would become so useful in these Covid times. [Below: N95 mask.]

Some people, mainly constitutional textualists and originalists, claim that governmental agencies such as NIOSH were not “intended” by the Founding Fathers, who could hardly have known about aerosols, viruses, or the Internet. Yet the Founders surely knew that knowledge, technology, and monetary systems were changing the world and would continue to do so – Franklin, Jefferson, and Hamilton most certainly among them. Enough Founders anticipated that American governmental regulation and American free enterprise would need to work in tandem to support the foundational principles of life, liberty, pursuit of happiness, and First Amendment protections. The NIOSH agency derives from any reasonable interpretation of the Declaration of Independence and the Constitution.
The global nature of human challenges, even for a matter so small as dust particles, is stunning. Airborne dust, solid or liquid, has no national boundaries. A NASA global simulation of aerosol transportation in the troposphere over 12 months beginning 17 August 2006, takes about two minutes to watch and will expunge any notions of national exceptionalism. This video clip shows that the recent African dust storm this year was no anomaly.
[Title: Atmospheric Aerosol Eddies and Flows – NASA GSFC S.ogv
Author: NASA. Date: 1 January 2008, 23:17:03]
On the other hand, the Covid component of respiratory aerosols is fortunately not very durable in time or distance. Infectivity seems to drop off after 6 feet or some number of hours. Otherwise, the above NASA animation would be very alarming in the face of this pandemic. Furthermore, the best evidence indicates that long-range transmission of small-particle aerosols (<5 micrometers) is not the dominant mode of Covid infection. Close-range respiratory droplets (large aerosol particles >5 micrometers) is the far more likely threat, easily thwarted by face masks and a little distance. [M. Klompas et al, JAMA, 324:441, 2020.]
Five.
Thermometry, a mainstay in the armamentarium of medical mousetraps, is a hot topic these days. Curiously, the fact of “normal human temperature” is not clear and some authorities believe that “normal” has been dropping. One wonders if normal temperature for communities of Inuit people living near the Arctic Circle is the same as “normal” of equatorial people, or could normal in infants be the same as for octogenarians? We don’t treat pulse or blood pressure with the same strict exactitude for all people, so why is 98.6 degrees Fahrenheit held to such precision, even though we know it’s variability in health is narrower than other physiologic parameters? Epigenetic response to modern life (industrialization, central heating, air conditioning, air pollution, global warming, etc.) surely influences the “normal” core human temperatures. Time of day, season, and age must matter as well. The site, method, and precision of measurement also effect any number obtained. 
The “normal” of 98.6 degrees Fahrenheit traces back to Carl Wunderlich (1815-1877), a German physician who questioned things (above, per Wikipedia). In 1868 he proposed 37 degrees Celsius as normal after studies using a foot-long thermometer, requiring upwards of 20 minutes to register the temperature. Surgeons may recall the term Wunderlich Syndrome, a nontraumatic surgical emergency of spontaneous retroperitoneal hemorrhage that may be caused by renal neoplasms. Mackowiak, Wasserman, and Levine in 1992, updated Wunderlich’s number. [JAMA 268:1578-80, 1992]. Newer studies suggest that “normal” human temperature has dropped by 0.59 degrees centigrade for men and 0.32 degrees centigrade for women. Urologists and zoologists know that core body temperature is a few degrees too warm for optimal testicular function in man, along with many other species, hence the “social distancing” of their placement. Evolutionary biologists may want to take note that as core body temperatures decrease, there may be no thermal reason for human testes to descend, which may severely limit the market for pediatric urologists. Kangaroos, and other creatures too, may have to adjust their testicular placement to accommodate themselves to a warmer planet (their bifid penile anatomy, caudal to the gonads, is stranger still.) [Below, Wikimedia, photographer and kangaroo unknown.]

Crises test all creatures, from viruses to humankind, forcing epigenetic changes that allow adaptation and evolution not only of individuals, but also their societies. Homo sapiens has taken this force of nature to unprecedented levels, but just as every new era brings out innovation, each challenge uncovers new generations of Flat Earthers who retreat to comforting beliefs, dogmas, and ideologies. In the arc of human progress, truth usually wins out and each crisis finds its own necessary technologies, although the arc of progress is not smooth, but often wobbly and intermittently retrograde.
Postscripts.
Summer reading. Caste, The Origins of Our Discontents by Isabel Wilkerson is a timely book. The title riffs on the first two lines and pun of Shakespeare’s 1593 play, Richard III: “Now is the winter of our discontent/Made glorious summer by this sun of York.” John Steinbeck echoed this in 1961 in the title of his final novel. Coincidentally, my summer reading also included the historical novel, Hamnet by Maggie O’Farrell, that imagined the lost life of Shakespeare’s only son (1585-1596). [Below: Title page First Quatro, Richard III.]
Caste (above) considers social and political power, but Wilkerson begins the book with “The afterlife of pathogens,” an astonishing coincidence with today’s pandemic news and world-wide political discontents. This first chapter describes a heat wave in the summer of 2016 that thawed Siberian permafrost and liberated anthrax spores from long-dead reindeer, thus causing a new epidemic in living reindeer and their indigenous herders, the Nedet people. Wilkerson then links that pathogen awakening to current political awakenings around the world.
“The anthrax, like the reactivation of the human pathogens of hatred and tribalism in this evolving century, had never died. It lay in wait, sleeping, until extreme circumstances brought it to the surface and back to life.”
Coincidences. G.K. Chesterton (1874-1936), English writer and author of the Father Brown priest-detective books, called coincidences spiritual puns. A less spiritual person than Chesterton might call coincidences cosmic puns or stochastic puns, but the idea is the same: unrelated but concurrent events or facts may seem to have been “divinely ordered” or happen “by the luck of the draw.” Chesterton’s actual quote comes from his book, Irish Impressions, in 1919, a year that coincides with the start of the first century of urology at the University of Michigan:
“All literary style, especially national style, is made up of such coincidences; which are a spiritual sort of puns. That is why style is untranslatable; because it is possible to render the meaning, but not the double meaning.”
Considering this first half of 2020, random chance is due to favor better luck in pathogens.
Thanks for reading Matula Thoughts this Labor Day, 2020.
Best wishes,
David A. Bloom