Matula Thoughts 6 November 2020
4129 words

One.
Autumn leaves and Nobel Prizes normally highlight this season, although Covid, climate, and a consequential national election dominated our attention this year. The award in Medicine or Physiology last month, however, went for discoveries relating to the hepatitis C virus.
That curious terminology of medicine or physiology is a historic reminder how science was disrupting health care when the Nobel awards began in 1901. A new certainty of physiology and other scientific disciplines, explaining the basis of normal biological function and disease back then, is now widely accepted in the 21st century, although we realize that the optimal practice of medicine in addition to its scientific basis also requires art and humanism. [Above: autumn leaves, Ann Arbor westside, 2020. Below: Nobel Prize medal.]
Politics are also in the air this month, even more unpleasantly than usual, and the Nobel awards are no less political than other human enterprises. Conflicts over these prizes have involved nearly all fields including that of Medicine or Physiology. The 1923 prize to Frederick Banting and John Macleod for the discovery of insulin outrageously excluded Charles Best and James Collip. Honorably, the two named prizewinners independently split their monetary shares with Best and Collip. No award was presented in 1925; the two main contenders, Johannes Fibiger and Katsusaburo Yamagiwa, had been proposed separately as the first to induce cancer in laboratory animals, but both were branded “undeserving” with great certainty by a key member of the award committee. Fibiger had used a roundworm he called Spiroptera carcinoma (Gongylonema neoplasticum) to cause stomach cancer in rats and Yamagiwa used coal tar to create cancer on rabbit ears. After further deliberation the following year, the prize went to Fibiger, although in durable fact Yamagiwa’s work was by far the better proof of principle of chemical carcinogenesis. Nonetheless, Fibiger was the first to get this Nobel Prize for work related to cancer. The second time this happened was in 1966 when Reed Nesbit’s first urology trainee, Charles Huggins, shared the award with Peyton Rous.
The Nobel Foundation offended Adolf Hitler when it awarded the Peace Prize in 1935 to Carl von Ossietzky, the journalist who exposed the clandestine German rearmament, illegal according to the Treaty of Versailles. von Ossietzky, a Roman Catholic, had been detained and beaten in German prisons and concentration camps since February, 1933, and was hospitalized with tuberculosis when the award was announced. Hermann Göring ordered von Ossietzky to refuse the award and the Nazi regime prevented travel to Stockholm but, in an act of civil disobedience, von Ossietzky issued a note accepting the Peace Prize. The ugly politics caused two committee members to resign and Norwegian King Haakon VII dodged the ceremony, even though the recipient could not attend. von Ossietzky died in 1938 while hospitalized under Gestapo surveillance.
In February 1953 Watson and Crick assembled an accurate model of the structure of deoxyribonucleic acid (DNA). Rosalind Franklin’s x-ray diffraction images, shown to Watson by Wilkins, provided the “eureka moment” in which the double helix configuration was realized. Watson and Crick were recognized for this with a Nobel Prize in 1962, that they shared with Wilkins. Franklin, however, having died of ovarian cancer in 1958, never learned of her role in the breakthrough and, by virtue of the rules of the Nobel Prize, was ineligible because she was no longer living.
Two.
[Above: Newton, by William Blake, 1805. Tate Museum.]
Certainty 1.0. Craving certainty, we derived it for most of human history from personal observations, beliefs, and the authorities of the times. A Matula Thoughts correspondent from Georgia raised the matter of moral certainty last month, quoting H.L. Mencken on the issue:
“Moral certainty is always a matter of cultural inferiority. The more uncivilized the man, the surer he is that he knows precisely what is right and what is wrong. All human progress, even in morals, has been the work of men who have doubted the current moral values, not of men who have whooped them up and tried to enforce them. The truly civilized man is always skeptical and tolerant, in this field as in all others. His culture is based on ‘I am not too sure.’” [Minority Report: H.L. Mencken’s Notebooks (1956).]
Morality and certainty, historically, were inseparable for most of humanity, hardwired in cultures and written into laws of churches, states, and organizations. Morality, as a topic, is far beyond scholarly consideration of this set of essays, but certainty is a matter of keen concern in health care. Philosophers, religious leaders, royalty, politicians, have offered their versions of certainty over millennia, but certitude challenges easy universal agreement, as one’s certainty on an issue is based on one’s origin, belief system, willingness to reason, and livelihood. Mencken, Lewis Sinclair, C.E.M. Joad, and others have variably said: “It is difficult to get a man to understand something, when his salary depends on his not understanding it.”
From a practical perspective as a physician, certainty means belief without rational grounds for distrust. Medical practice demands that conclusions must be drawn with certainty, for example, from urine specimens whether in matulas, under microscopes, via chemical strips, or on culture plates. Urologists, as all practitioners, depend upon certainty in diagnosis and therapy, yet we cannot be absolutely certain about everything that passes under our visage. Relative certainty is a practical and essential qualification. [Below: Constantine examines urine in matulas. 11th c. Wikipedia.] 
Mencken (1880-1956), influential journalist and social critic known as the Sage of Baltimore, could turn a phrase well, but he represented a peculiar elitism and exceptionalism of the first half of the American 20th century. Self-assured in his certainty, he often was acerbic and dismissive to those he perceived as lesser intellect or “lower caste,” although he didn’t use that terminology. Mencken was contemptuous of Franklin Roosevelt, argued against the New Deal, objected to U.S. participation in WWII, and harbored admiration for the Nazi regime. Ayn Rand was one of his great admirers, but other influential voices were critical. Christopher Hitchens later offered a scathing opinion of Mencken in a book review.
“How did one of America’s seemingly great rationalists and modernists come to regard Roosevelt as more worthy of condemnation than Hitler? The answer, on the evidence of this and other studies, is that Mencken was a German nationalist, an insecure small-town petit-bourgeois, a childless hypochondriac with what seems on the evidence of these pages to have been a room temperature libido, an anti humanist as much as an atheist, a man prone to hyperbole and sensationalism he distrusted in others and not as easy with the modern world and its many temptations and diversions as he liked it to be supposed.”
Hitchens also turned his phrases well, but when he hit, he struck hard and unsparingly. [Hitchens, “A Smart Set of One,” The New York Times (17 November 2002), book review of The Skeptic: A Life of H. L. Mencken (2002) by Terry Teachout.]
Certainty, although personally comforting, closes the mind to new ideas and leads to smugness. It is irrational to expect 7 billion people to share the same certainties about all matters, short of a limited number of generally-accepted facts, such as that days follow nights, the moon has phases, eclipses occur occasionally, kindness and civility are nice, and some things such as infanticide and cannibalism are grotesque. The first rule of certainty, however, is that change is inevitable and accordingly, uncertainty rules above all.
Three. 
Uncertainty. Werner Heisenberg made uncertainty respectable when his concept of indeterminacy (on a very small scale) in 1927 garnered him the 1932 Nobel Prize. Erwin Schrödinger carried the idea to the visible world in 1935 with his famous thought-experiment and paradoxical cat. [Above: Heisenberg c. 1901; Below: Schrödinger c. 1933. Wikipedia.]

[Above: Movable silhouette of Schrödinger’s fictional cat in the garden at Huttenstrasse 9, in Zurich where he once lived; visitors outside the walls cannot know the cat’s position or its direction, at any moment. Wikipedia.]
Uncertainty entered the moral dimension and popular culture, it could be argued, with Bryan Cranston’s fictional character Walter White in the Vince Gilligan television series of 2008. White, a modern-day high school chemistry teacher, is followed over five television seasons “breaking bad” into a dark world of the manufacture and distribution of 96% “pure” methamphetamine. White’s nickname Heisenberg initially conveyed his good state as a brilliant chemistry teacher, but the full irony came out when Walter turned to his dark side as a meth kingpin. [Below: Breaking Bad publicity still, Walter White.]
Mencken’s caution of self-certainty and promotion of “I’m not too sure” belied a number of other outrageous statements, defaulting to intemperate self-certainty, and forgetting his own restraint of “I’m not too sure.” Some Menckenisms reflected primal certainty that trumped morality and civility, such as “Every normal man must be tempted, at times, to spit upon his hands, hoist the black flag, and begin slitting throats.” [Mencken, The New Poetry Movement, Chapter 6.] [Below: Jolly Roger Flag.]

Momentary reversion to the primitive pirate in everyman – casting off the morality and mores of humanity, whether in thought-experiment or actuality – can’t be blamed on Mencken. He articulated the idea well, but it hardly originated or ended with him, and homicide remains widely evident in fact and fiction; even if we do not choose to be murderous outlaws, we relish them in our entertainment.
It comes as a surprise, now, 20 years into the 21st century, to find widespread craving for authoritarian rule. Possibly, this is propelled by a growing sense of nihilism where too many people prefer the certainty of “I don’t really care except for what’s good for me” over the uncertainty of “I’m not too sure.”
Four.
Independent thought. Modern society seemed to be gravitating toward the intellectual relativism of “I’m not too sure,” although maybe that was my wishful thinking.
It is reasonable to believe that throughout human history most people prayed for relief from authoritarian subjugation by clan leaders, priests, pharaohs, princes, kings, queens, and dictators. Those few leaders dictated their personal certainties to everyone else, claiming authority derived from physical strength, bullying, divine authorization, bloodline, caste, national exceptionalism, political sectarianism, or other “isms.” Physical intimidation in authoritarian societies suppresses expression of uncertainty and even more effectively, the memes of sectarian “isms” act as ideological viruses replicating the certainty of patterned thoughts in individual minds and crowds, precluding reasoning and doubt.
People, perhaps most, chafe under authoritarian rule, although they may do so silently. The contrary meme of the pirate, openly rebuking authority of the establishment, always finds sympathy in regulated societies, even those not authoritarian and repressive. An interesting example is the island of Corsica, variably contested by many authoritarian nations over the centuries and now French, proudly displays its counter-cultural pirate symbol on flag and coat of arms. [Below: Corsican symbols of independence.] 
Mental acrobatics that lead to certainty are sometimes called heuristics and, aside from crude mapping by functional MRI, the neural gymnastics at play defy our best imagination and science. It is more convenient to be told what things are certain than to be figuring them out in every step of life’s way. Our historic predecessors – early humans lacking today’s sharpened tools of logic, science, and debate – must have found comfort to be given explanations for solar eclipses, earthquakes, or monsoons by tribal leaders or village priests, rather than tremble at the uncertainty of it all.
The problem with human thinking nowadays seems to be the matter of how people deal with their sense of “I’m not too sure.” Methodological thinking, analysis of information, and fair discussion can help people understand what to be sure of, what to question, and how to decide. However, these instruments of education, science and free speech are only effective when we step outside the comfort of our particular certainties and open our minds to other opinions, information, rational debate, and experiments of thought and science. Too often, we revert to the easier dogma of our sects and certainty our leaders.
The Good Doctor, a new book by our Georgian colleague, examines the importance of uncertainty in medical practice; no good physician can be a know-it-all. On the other hand, nobody wants an ambivalent doctor who offers a list of ten possible diagnoses and ten potential remedies and tells us to choose what we prefer. [K. Brigham, M.M.E. Johns, The Good Doctor, Why Medical Uncertainty Matters. Seven Stories Press, NY, 2020.]
A relevant thought comes from professor Sarah Buss here in the UM Philosophy Department who explains to her students that they can’t gain a deeper understanding of issues they consider in class without becoming less certain where they stand on those issues: “I aim to help them gain clarity, knowing that the result will often be a loss of certainty.” Professor Buss, in turn, quotes colleague Kieran Setiya:
“The patience to ask and to keep asking questions, without the assurance of agreement or the availability of methods apt to elicit it, is the philosopher’s gift. It is an expression of intellectual hope, and the repudiation of philosophy is a counsel of despair.”
[K. Setiya. Monk Justice. London Review of Books. 42 (16), 30 Aug. 2018.]
For everyday events on the human scale, in space and time, things are usually one way or another. We are used to uncertainty in life, but we prefer predictability, whether in elections, horseracing, or surgical outcomes. In fact, we depend on some degree of certainty, even if it is the probability of knowing the odds of a specific throw of dice or hand of cards, assuming fairness of the event. Statistics for a condition or certain state within a group, however, doesn’t translate well to a particular person for whom having the condition or state is a personal possibility of “yes” or “no,” that is a 50% probably in their mental calculus.
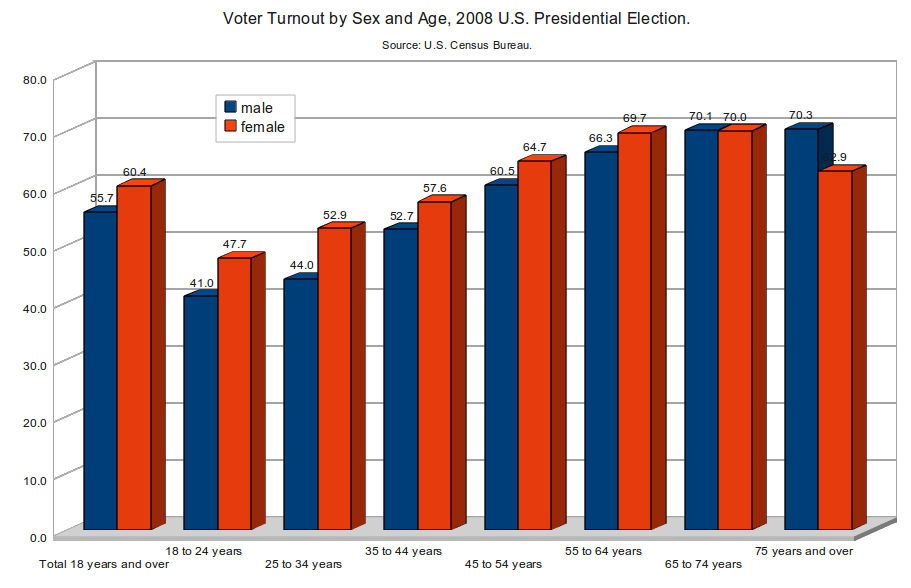
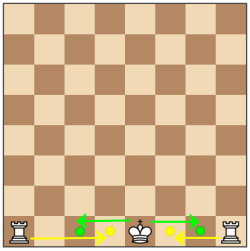
Adjectives and numbers help arbitrate uncertainty. Even simple adjectives, as in the world of genetic diseases, may offer precision. For example, “rare” conditions are said to affect less than 62/100,000 people while “ultrarare” has come to mean fewer than 2/100,000. [J.M. Friedman et al, “Exome sequencing and clinical diagnosis,” JAMA, 324:627, 2020.] By this terminology hypospadias is not so rare (2 in 500 male births), while cloacal exstrophy is ultrarare (1 in 250,000 births). A recent zoom visiting professorship to our pediatric urology division from Katherine Hubert Chan of Riley Children’s Hospital, offered a lesson on graphics in surgical decision-making, utilizing icon arrays to demonstrate frequency of a given condition. Pictographs nicely convey a sense of likelihood or unlikelihood without the abstruse jargon of high-voltage statistical tools. [Below: an icon array.] ![]()
Five.
Certainty 2.0. At some point we humans admitted a new form of certainty into our minds, basing belief on rational argument, verifiable evidence, and experiment, rather than anecdote and authority. Paradoxically, this new certainty is based on acceptance of some uncertainty that facts and models change as we interrogate them. Nonetheless this should not allow a lazy retreat to anarchy and nihilism where nothing is held true.
Certainty is desirable in surgical practice; when treating stones, congenital malformations, or malignancies, specific identification of a problem is closely linked to beneficial solution. Yet knowledge and technologies change and yesterday’s certainty becomes today’s uncertainty, thereby reintroducing the questions, how do we know what is correct and how should we act today?
Hugh Cabot, founder of urology at Michigan and man of great certainty, took wide interest in medicine, often crossing epistemological boundaries to study and collaborate outside of his field. Working with pathologists on a paper on gastric cancer in the era of the Nobel controversy, Cabot and fellow faculty member George Adie had published their thoughts on its etiology in 1925, quoting views of their colleague, Aldred Warthin. [H. Cabot and G. C. Adie, “Etiology of Cancer of the Stomach,” Annals of Surgery 82 (1925): 86–108.] William Mayo, another physician with an Ann Arbor connection (UMMS, 1883), was also interested in the topic, writing a lead article in Surgery, Gynecology and Obstetrics in 1912 that discussed treatment from his point of view: “Cancer of the stomach: its surgical cure.” [SG&O, 14 (2): 115-119.] Mayo criticized lengthy diagnostic interludes that allow the disease to progress from “week to week” until by the time a practitioner has absolute certainty of the diagnosis before referring to patient to Rochester, “This is not a case for the surgeon, but for the undertaker.” Mayo concluded: “Cancer of the stomach is the most frequent and most hopeless form of cancer in the human body. Early operation affords the victim the only chance of a cure.” Time and discovery have altered the certainty of those conclusions. Ironically, gastric cancer took Mayo’s life at age 78.
The rapidly changing conditions, information, and misinformation surrounding Covid-19 have challenged medical certainty and public certainty. Political iniquity and social media mischief accelerate the uncertainty and miscertainty. Rather than dwell on this here, we offer two essential articles from NEJM, both accessible at no charge on the internet.
One editorial says it all. “Dying in a leadership vacuum,” [NEJM, 2020; 383:1479-1480.] A perspective by J.N. Rosenquist, “The stress of Bayesian medicine – uncomfortable uncertainty in the face of Covid-19.” [https://www.nejm.org/doi/pdf/10.1056/NEJMp2018857?articleTools=true]
Postscript.

Frank Legacki, legendary Michigan Swim Team Captain of the Class of 1961, successful businessman, and friend of the University of Michigan Musical Society and Department of Urology, passed away last month on 10/16/2020, leaving his wife, Alicia Torres. [Above: Frank at Steve’s Deli, September 23, 2020.]
Born 9/28/1939, Frank grew up in a tough Philadelphia neighborhood, the oldest of eight children – six boys and two girls. His parents, of modest means, believed in education and raised the children firmly and proud of their background and opportunities. Dad, a Polish immigrant, was a carpenter. Mom, daughter of Irish immigrants, deftly managed the large family. Frank attended Father Judge High School, where by luck and hard work, joined the rudimentary swimming team his freshman year. Lacking a pool at the school, Frank and teammates trained at pools as much as 1.5 hours away. Swimming was the glue that kept him focused in high school and he became a National Catholic High School Champion and a Scholastic All-American, earning athletic scholarships at several universities. Narrowing his choices to the University of Michigan and Ohio State University, both with top Collegiate Swimming programs, Frank asked his high school coach which school to attend. The coach answered, “Probably Ohio State, Michigan is far more difficult academically and you may have problems getting through at Michigan.” Frank decided on the spot to go to Michigan.
Education and swimming at UM shaped his life. Eligible for the team in his sophomore year, 1959, Frank became NCAA Champion in the 100-yard freestyle and anchored the winning 400-yard freestyle relay. Two weeks later at the US Open Championship (later called the National AAU Championships) he set the American record in the butterfly. Michigan’s score of 95.5 at that competition was a new record and solidified the UM 1959 Swim Team as the greatest in NCAA history. Frank and his team continued to win and set records, and he was elected captain in his senior year, receiving other honors and leadership positions outside of athletics. Frank married after graduation in 1961 and stayed in Ann Arbor for an additional year to get an M.B.A. The couple would have four daughters, divorcing after 23 years.
A business career took Frank to New York City at Ogilvy & Mather Advertising. He went on to executive positions as: Managing Director of the Strategic Consulting Group of Marketing Corporation of America; VP of Marketing for Converse Athletic Footwear; Founder and President of the Andover Consulting Group; and President of Kaepa Athletic Footwear. Frank led a buy-out of this last company and eventually sold Kaepa to Umbro Sports Apparel. During these years he returned to UM for an M.B.A., graduating in the top quarter of the class.
In the business world Frank met Alicia Torres in San Antonio in the autumn of 1993 and they became business friends and then partners. Organizing a leveraged buyout of software products, and they formed Rosebud Solutions, generating outside investments, building a skilled team, and growing the business. Their partnership became personal and they grew close, marrying in Philadelphia on August 8, 1998, and then relocating in Ann Arbor. Rosebud was acquired by McKesson, Inc. (NYSE: MCK) in 2008. Frank went on to work part-time with Fletcher Spaght, Inc., a Boston venture capital firm, eventually retiring fully.
Frank, always loyal and grateful to UM, often said: “I was born at the University of Michigan; it was here I learned how to think.” In Ann Arbor, Frank and Alicia immersed themselves deeply in university matters and the community, enlarging their network of friends and interests. Frank was recognized for his achievements by induction into the University of Michigan Hall of Honor and The Pennsylvania Sports Hall of Fame. He stayed active with the University as President of the Grey Whales (Swim Boosters); Board of M Club Letter winners; UM Alumni Association Board; UM Urology Department Board; and Chair of the Marketing Committee of the University Musical Society. Frank was also President of the Barton Hills Maintenance Corporation. Frank and Alicia regularly attended over 20 UMS performances annually as well as School of Music Theater and Dance events. They generously supported Michigan Theater and were regular presences at UM athletic events, with season tickets for Football, Basketball, Hockey, Wrestling, Softball, and Swimming meets. Active fishermen, they cast lines in Florida and exotic locations around the world. Frank loved his time with grandchildren, Sam, Sophia, and Noah, taking them fishing, to UM events, and cooking together. The kids loved “GP Frank.”
Frank shared his rich and full years generously with friends, family, neighbors, and the University of Michigan. Alicia recounts:
“Frank had an amazing life. He gave much more than was given to him, and celebrated life like very few. He loved keeping in touch with elementary, high school, and college friends and those he met during his career and travels. Frank asked strangers about their life, where they were from and then, they too became Frank’s friends. Through his travels, Frank always carried an extra U of M cap, which he would give to people who captured his heart. When Frank entered a room, he owned it, you knew he was there, in a good way.”
Paul Legacki from Sacramento, Frank’s last living brother, was a frequent visitor to Ann Arbor in Frank’s final year. Frank anticipated his final days gracefully and with good humor, requesting his epitaph be borrowed from the last lines in Edmond Rostand’s great play, Cyrano de Bergerac. In the final scene Cyrano lies in Roxanne’s arms, mortally wounded and weakening, as he looks at Roxanne and says his final words; “They have taken my life, but they have not taken my panache.” Frank lived an active and interesting life, with extraordinary panache.
In one of the sweet coincidences of life, the lovely home of Frank and Alicia is situated exactly between those of Ananias Diokno (Nesbit 1970) and Kate Kraft (Nesbit faculty 2011), and across the street from the former home of Ed McGuire who succeeded Nesbit’s direct successor as Urology Section Chief in 1983, Jack Lapides (Nesbit 1950). Ananias and Kate’s family looked over Frank in his last days. Many of us lost an extraordinary friend when Frank died. His passing, at a young and robust 81 years of age of metastatic prostate cancer, reminds us painfully that we still have a long way to go in our work in urology.
Additional Postscripts.
The Lasker Awards were held back this year due to the Covid-19 pandemic. These are awarded annually since 1945 to living persons who have made major contributions to medical science or performed public service on behalf of medicine. This year the Foundation instead highlighted the 29 awards given in the past that recognized advances in infectious diseases, the first of those going to John F. Mahoney in 1946 for treatment of syphilis with penicillin and the most recent to Douglas Lowy and John Schiller for vaccination to prevent HPV in 2017. [J.L. Goldstein, JAMA September 25, 2020.]. My bet for a 2021 Lasker Award will be on Anthony Fauci for his tireless and courageous representation of scientific truth in the public interest in turbulent times.
Apocryphal Keynes quotations: “When the facts change, I change my mind. What do you do sir?” or “When someone persuades me that I am wrong, I change my mind. What do you do?” Variants of these have been attributed to redoubtable British economist John Maynard Keynes (1883 -1946), but no direct sourcing has been found. Nobel laureate Paul Samuelson and others alluded to versions of the remark, long after Keynes died. Whatever actual the source, it is an enlightened human idea.
True fact. Face masks diminish respiratory germ transmission by respiratory droplets. This is certain and has been clear to every surgeon, nurse, and OR worker on the planet for well over a century. Argument on this point is futile and malintented. 
[Above: Justin Dimick and Hari Nathan, UM Surgery Department. Below: Aditya Pandey & Paul Park UM Neurosurgery Department.]

Thanks for looking at Matula Thoughts this November, 2020.
David A. Bloom
Department of Urology, University of Michigan