WN/Matula Thoughts April 2, 2021
Showers and shows, corvids and covids
2,765 words
One.
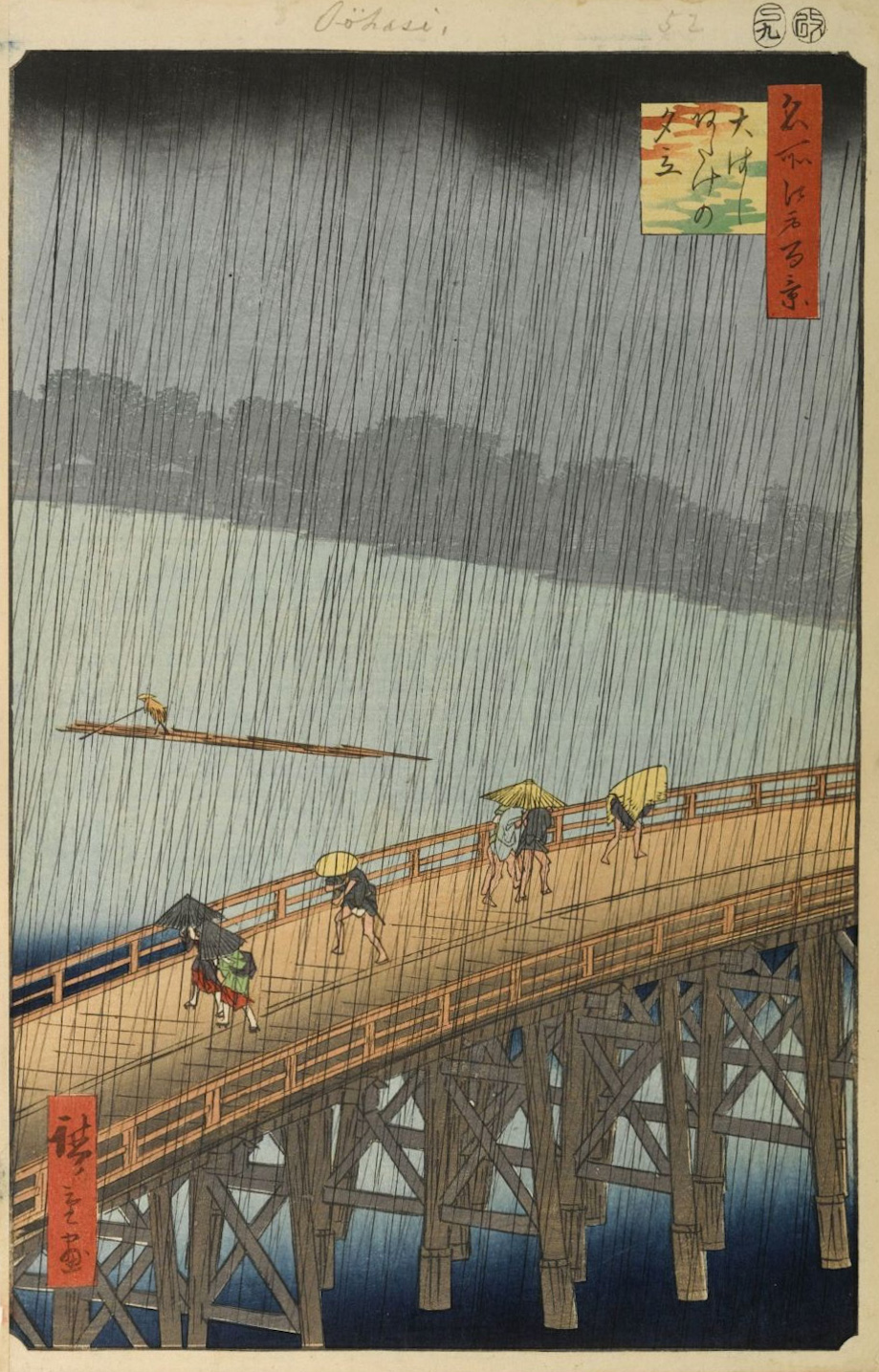
April showers are annoying when they catch you unprepared but these heavenly shows can be enchanting and do bring May flowers. Spring rains entertain and sometimes astonish with their beauty, intensity, and lightning spectacles. Most importantly April showers are essential to the planting seasons that we humans have relied upon for 7,000 years.
Painted the same year as Hiroshige’s Sudden Shower (above) is Millet’s The Gleaners, showing three women gleaning a field for stray stalks of wheat (below) on a cloudy day before crows and other animals picked them off. [Two paintings from 1857. Above: Utagawa Hiroshige’s Sudden shower over Shin-Ohashi Bridge and Atake in the One Hundred Famous Views of Edo series. Brooklyn Museum. Below: Jean-Francois Millet’s The Gleaners, Musée d’Orsay.]

Agriculture, the invention essential for human success, also expanded opportunities for the adjacent success of predators of both our foodstuffs and increased populations. Modern society, interconnected and mobile, in turn offers easy opportunity for global distribution of viral predators by aerosols and droplets to 7 billion human incubators that further disseminate and revise the predator.
Inventions have kept us ahead of extinction so far and scarecrows were one of the better early inventions, arguably our first robotic impersonators, animated by the wind as they waved off corvids and other winged diners.
The Covid pandemic (declared last spring on March 11) reminded that our food supply remains tenuous – whether threatened at the source by predators or by supply chain breakdown – with bare shelves in the aisles of food stores a year ago. Food security now more than ever is at risk because of the intricate supply chains of modern society – contingent on geopolitical, economic, and biological stability. Just now, the inventions essential to survival are vaccines.
Human cooperation using masks and prudent distancing and the incredible ingenuity of vaccines – their amazing creation, mass production, and deployment in less than a year – may lead us out of this crisis and give time to prepare for the next one. Whether the next challenge will come from the likes of corvids or covids remains to be seen, but challenges are to be expected.
All nations stumbled in terms of pandemic response, some more than others. We debate which political party or political system will best protect us from the next disasters, but it is more likely that a balanced portfolio of domestic political parties and international political systems in relative harmony will offer the best chance. No single ideology – libertarian, democratic, republican, socialist, parliamentarian, monarchy, corporatocracy, etc. – is likely to offer the best hope for mankind, although representative democracies with fair open societies are more likely to bring innovation to the forefront and extract the optimal wisdom of crowds than other systems.
Two.

April hosts other celestial shows, notably the Lyrid meteor showers (April 16-26) with an average count of 10 meteors per hour, providing spectacular night-time shows at this time of year (above). Rainstorms and meteor showers, as parts of nature’s pageantry, entertained humanity long before we learned to create our own shows, through stories, visual art, song, and playacting. [Image credit: Astrophotographer Mark Lissick. Lyrid meteors and the Milky Way, taken on April 22, 2013, in Hope Valley, California (near Lake Tahoe). Mark Lissick/Wildlight Nature Photography.]
Modern life, especially during these days of Covid, has pushed much of our entertainment indoors to the small screens of households and personal devices. News, commentary, biography, history, and drama – and various mixtures of these – provide more than enough “content” to entertain and educate us when leisure time crops up between the moments of getting our daily bread and preparing it.
One year ago, Covid-19 was exhausting hospital and mortuary capacities around the world, schools and restaurants closed, and unemployment exploded, although large chunks of the population refused to believe those facts and reports. Social isolation forced new approaches to work, education, and entertainment. Fear and the paradoxical echo-chamber news of social media magnified primitive challenges to social cohesion, public safety, and science. These challenges are to be expected in a free society – mask doubters, vaccine refusers, and violent extremists have been around since the last major pandemic – but it seemed worse with this pandemic. The contrarian support from political leaders, however, was not only a low moment for this democracy, but it was consequential in terms of exacerbation of lives lost from unnecessary congregation and virus dissemination but also humiliated this nation in the view of other nations.
Three.
Small screens. Social isolation forced most of us indoors for work and entertainment while the internet and innovative software allowed immediate access to workplaces, education, news, and recreation around the clock and throughout the week. People and families worldwide who were lucky to have home televisions or devices with internet capability, self-entertained at an unimagined scale. Motion pictures were already in the process of transitioning from public theaters to mobile devices, but the pandemic accelerated the transition. [Below: Peepa Pig © and her family watching TV.]
Medical topics have entertained people throughout the history of modern literature and early in the 20th century. Plays such as Shaw’s The Doctor’s Dilemma (1906) and novels such as Arrowsmith by Sinclair Lewis (1925) remain relevant today, reflecting cultural attitudes and issues of their times and ours. After written plays and novels translated to motion picture shows the genre burgeoned in the later 20th century and expanded to this century, admixing entertainment with social commentary on cultural attitudes, personal crises, ethics, and injustices reflecting myriad facets of the human condition. To me, the greatest medical story in print, from the perspectives of authenticity, plots, and style, is Cutting for Stone, by physician Abraham Verghese (2009). It leaves most others far in the dust.
A complete examination of the medical stories in print, on stage, and on screen would be a larger project than would be suitable here, but a cursory view of health care shows for personal entertainment at home, is entertaining in itself.
Four.
The first popular TV medical shows featured characterizations of generalist physician Dr. Kildare (1961-1966, five seasons, 191 episodes) and a brilliant and thoughtful neurosurgeon Ben Casey, MD (1961-1966, five seasons, 153 episodes). They are long gone but the soap opera General Hospital endures (1963 – present, 47 years over 14,000 episodes), with a brief disruption for Covid, offering romance, marriages, mistresses, mayhem, crime, and episodic murders broadcast in an afternoon time-slot. Medical shows have burgeoned and this list is hardly comprehensive, but illustrates the spectrum and chronology. [Below: BBC image from 1966.]

Marcus Welby, M.D. (1969-1976) returned to the theme of a kind family doctor solving common physical and emotional problems in a small town over a gentle range of social issues while dealing with his own family’s dramas. This was the first ABC show to become #1 on TV (in its second season 1970-71), lasting for seven seasons with 169 episodes.
Realism mixed with comedy in M.A.S.H. (Mobile Army Surgical Hospital) as a medical team in a combat zone (actually Korea and watched in the context of Vietnam) lightened its daily load of tragedy and pathos by comedy. Based on a 1968 novel by Richard Hooker and a 1970 feature film, M.A.S.H. was translated into a half hour television series on CBS that lasted 11 seasons with 256 episodes from 1972 -1983. The dark comedy brought gallows-like humor to the serious business of the operating theater.
St. Elsewhere (1982 -1988) also carried realism into living room TVs with dramas of a medical team in an underserved community for six seasons with 137 one-hour episodes that earned critical acclaim and concluded with a brilliant ending.
Doogie Houser, M.D. (1989 -1993) mixed the challenges of hospital-based medical practice by a boy-genius leukemia survivor who, at age 14 had become the youngest licensed physician in the U.S. The show begins with him at age 16 as a surgery resident in LA, living at home with his parents and follows him for 97 episodes dealing not only with his obvious precocity (he can prescribe drugs but can’t buy beer) as well as inner city gang trauma, racism, AIDS, homophobia, etc. Created by Steven Bochco and David E. Kelley. Doogie Houser was an unlikely successor to Steven Bochco and David Milch’s Hill Street Blues (1981-1985).
Dr. Quinn, Medicine Woman (1993-1998) offered a new take on medical dramas, featuring a woman physician placed in the American west, spun out into six seasons, 149 episodes, and two television movies.
E.R. (1994-2009) incorporated the dramas and personalities at play in a large city Emergency Department. Created by physician Michael Crichton the long-running show established the careers of some notable actors and the idea of this new subspecialty of medicine as a lifelong career path in the eyes of the public, for until recent times Emergency Rooms were usually staffed by rotating trainees, generalists, and on-call specialists. This lasted 15 seasons with 331 episodes.
Bramwell set in late Victorian England follows Dr. Eleanor Bramwell, challenging men and stereotypes as she runs a hospital for the indigent she calls The Thrift, in the East End of London beginning in 1895. This British show lasted for four seasons with 27 shows between 1995 and 1998, and still holds up well to modern viewing. [Below: Sony “flat screen” TV from 2000.]

Twenty-first century small-screen shows revised reliable old themes but also ventured deeper into less complimentary and comforting themes of medical practice including commercialism and more nuances of human behavior and social context.
City of Angels (2000-2002) ran for two seasons with 24 episodes on CBS. It was the first main network medical drama with a predominantly African-American cast.
SCRUBS (2001-2010) was a heroic diary of a young physician, produced by Disney, lasting for nine seasons with 182 episodes.
Nip/Tuck (2003-2010) dramatized the business of cosmetic surgery with comedy and drama, lasting for six seasons and 100 episodes.
House (2004-2012) portrayed a brilliant Sherlockian diagnostician with his own problems. He was a notorious rule breaker but solver of medical mysteries that confounded others. Counter-intuitively misanthropic and dependent on pain medication, the lead figure Dr. House was played by actor Hugh Laurie, son of a well-known English physician, Ran Laurie. The actor later said he felt guilty for being paid more money to portray a fake version of a physician, than his father ever earned as a real physician. This highly acclaimed show lasted eight seasons with 177 episodes. [Wikipedia.]
Doc Martin (2004-2021) tells the story of a quirky vascular surgeon at Imperial College London who develops hemophobia and relocates to a small Cornish village, where his uncle and aunt own a farm. Doc Martin readjusts his career to become a general practitioner although the antithesis of the kindly Marcus Welby phenotype. Dr. Martin lacks any bedside manner – lacking social skills he is rude, abrupt, and generally unkind for nine seasons and 70 episodes usually of 50 minutes.
Grey’s Anatomy (2005 – ), produced by Shonda Rhimes, centered around a young woman physician named Meredith Grey, punning on the classic anatomy textbook of Henry Gray of 1858. Meredith’s dramas began with her as a surgical resident in Seattle and the prime-time show lasted for 17 seasons with 370 episodes up to the pause for Covid.
Nurse Jackie (2009-2015) ran for seven seasons and 80 episodes, featuring an emergency department nurse in a NYC hospital. The show explored difficult issues including drug addiction and The New York State Nurses Association protested perceived “unethical behaviors” of the main character in bending rules to best serve patients.
The Knick (2014-2015) ran only for two seasons with 20 episodes in a fictional Knickerbocker Hospital in NYC around 1900. The protagonist, Dr. John Thackery, was the chief of surgery modeled on William Halsted balancing his own drug addiction with ambitions for innovation and excellence. Economic stability of The Knick, racism, and ethical issues contend in the plot of this historically realistic show, which was deeply informed by Dr. Stanley Burns and the Burns Archive.
It would take a larger essay to encompass all the other medical television shows, especially the new ones that are proliferating with melodrama, excitement of the operating room and emergency department, stereotypes noble and vile, including: Chicago Med, The Resident, Transplant, Virgin River, Trauma, 9-1-1, Valkyrien, Nightshift, New Amsterdam, and others. Historical themes returned with The Knick and a truly bizarre show, Ratched, imagined a prequel to the notorious psychiatric Nurse Ratched from the great film One Flew Over the Cuckoo’s Nest. All these shows leave little doubt that the genre will continue, portraying a broad swath of the human condition through healthcare lenses. If another global quarantine comes by, these shows offer 2,436 episodes to binge – even before turning to the enduring soap opera, General Hospital, with its more than 14,000 stories.
The bottom line is that the medical shows have specialized into as many different versions of the profession and its professionals as the public has experienced or can imagine – from the finest to the basest. Many shows inspired countless young people towards health professions from Dr. Kildare, to M.A.S.H. to Nurse Jackie. [Below M.A.S.H. season six cast.]

M.A.S.H. more than most other medical shows revealed the systems behind the personal dramas of each episode, and the imperfect and often contradicting systems of the U.S. Army added to the complications of each day. Military medicine is a vast set of services and supply chains that may need to be mobilized and moved across the planet at a moment’s notice. Yet this is but one part of the national “health care system” at play on a 24/7 basis.
Five.
Documentaries. Of all types of shows, documentaries are the most compelling for me, showing the world and ourselves (in the larger sense) to ourselves in the personal sense, with the good, bad, ugly, and beautiful of life. Health care documentaries are a rich genre and a good place to start is Crip Camp. Camp Jened was a summer camp for children with disabilities that began in 1951 and was recently explored in a film by James LeBrecht and Nichole Newnham that won the Audience Award at the Sundance Film Festival in 2020 and an Oscar nomination (available on Netflix). LeBrecht began Camp Jened himself in 1971 and his film, with archival footage, tells how a cohort of campers came together in their later lives to join in social actions that informed broader social understanding of what George H.W. Bush would call “the shameful wall of exclusion.” Bush used that phrase when he signed the American Disabilities Act in 1990. The role of the Crip Campers was essential to that story and the film will broaden your understanding of the idea that human freedom – encompassing life, liberty, and the pursuit of happiness – is intrinsically tied to personal health with mobility and access to fair inclusion in the world.
Health and healthcare, equitable and excellent, are great aspirations of human civilization – just as are clean air, good water, and food, along with shelter, public safety, and human liberty. No deity, divinely authorized authority, or algorithm provides these things. Multiple nations, regions, local authorities, and organizations must provide these things for their stakeholders. The public complaint that “the health care system is broken” implies an expectation that an actual system should exist, whereas in fact multiple systems are at play often at cross purposes nationally and internationally. Expecting a government or political party or algorithm to create a perfect system (or “fix” a “broken” one) is a fool’s errand. The solution will be to optimize performance and coordination of the myriad organizations through wise legislation, robust and fair safety nets, responsible corporations and unions, honest professions that serve the public, and an educated public.
Professions have been at the heart of health care, notably the early profession of healing or medicine documented since Hippocrates and the more recent profession of nursing, so well codified by Florence Nightingale. The corporatization and industrialization of health care, while necessary and inevitable at some levels, have eroded the professions that have humane aspirations rather than economic and metric motivations. Retention of a balance between profession and industrialization in the delivery of health care may be the best hope in constructing a set of health care systems for the future.
Postscript.
Truth and fiction. Journalism, personal memoir, factual narratives, and documentaries declare themselves to tell truth but is the marketplace of the readership that validates the claim. Fictional stories as works of imagination are rooted in actual human experience and, at their best, tell truths. These narratives of imagined stories may achieve realism through their art, uncovering truths and sometimes displaying them with astonishing clarity – the truth of a moment in life, a scene, a person, or a story. For these works too, the marketplace of readership validates the authenticity. In fiction or factual narrative, health, disability, and disease will always be compelling parts of our stories, however they are told, illuminating for better or worse the human condition, as it is called.
Thanks for reading Matula Thoughts this April, 2021.
David A. Bloom
University of Michigan