DAB What’s New Feb 1, 2019
![]()
Sands of time, transition, & short thoughts on rules
3996 words

One.

February, the shortest month, begins today, this Friday, and its periodic extra day comes next year on a Saturday. Although 2019 is only a month old, the sands of time slipped away for one iteration of Michigan Urology, and the metaphorical hourglass reloads today for our Michigan Urology version 8 that will refresh our department. Regental privilege requires that the next urology chair requires formal action, although most of us know the party in question, who begins today as acting chair. Ganesh Palapattu will do an excellent job leading the faculty, residents, and staff – the parties who will actually do the refreshing. Our new chair will face challenges and, if history is any guide, our team will support him fully for the next chapter of the Michigan Urology journey. In that context, this is a good time to examine the past and re-articulate our history, as Richard Feynman (1918-1988), American theoretical physicist, once wrote:
“Why repeat all this? Because there are new generations born every day. Because there are great ideas developed in the history of man, and these ideas do not last unless they are passed purposefully and clearly from generation to generation.” [Feynman RP. The Meaning of it All. Thoughts of a Citizen Scientist. 1998.]
It may be a long stretch from the “great ideas in the history of man,” to a modest history of Michigan Urology but I hope you allow Matula Thoughts some slack and accept this belief in regularly rearticulating the past for each cohort of our successors.

I first met Ganesh when I was visiting professor at UCLA, my urology alma mater, and he was a resident under Jean deKernion, a wonderful urologist, leader, and friend. As a visiting professor at a number of places, I often tossed out ideas for papers, but Ganesh was perhaps the only one over the years who took the bait and completed a paper with me. His career took him to Johns Hopkins, The University of Rochester, and then Baylor in Houston at Tim Boone’s program. At great loss to Tim, but with his consent and blessing, Ganesh and his lab, with Alex Zaslavsky, came to Michigan at the start of my term as chair. Ganesh is well prepared. He is a terrific teacher, effective leader, excellent surgeon, and has led our largest urology section, uro-oncology, very well. When a need is identified he steps up – he was among the first to volunteer in Flint at the Hamilton Community Health Network clinic, when that opportunity materialized. His lab has done well with a recent 2% score on its latest grant submission. Ganesh will be thoughtful, consensus-building, and creative as he leads Michigan Urology in its mission (education, research, and clinical care), and our essential deliverable – kind and excellent patient-centered care. [Above: Ganesh with Anu. Below: with Kirtan and Elina.]

Two.

Anticipating the centennial of Michigan Urology, we’ve been working on a new volume of our story, previously written by the late John Konnak and urological scholar Dev Pardanani nearly 20 years ago. It is impossible to understand the urology story in Ann Arbor, without a larger sense of the story of our state, our specialty, and our university. It might be said that melodies of the past haunt the reveries of our stories, to tweak Hoagy Carmichael’s phrase. So, our story properly began around 11,000 years ago, well before Hippocrates and the known roots of medical practice, with the inhabitants of the Mound Builder and Woodland cultures who populated our geographical area after the last glacial period receded. The Holcombe beach site near Lake Saint Clair has evidence of Paleo-Indian settlement in that era and by the 17th century, Huron, Odawa, Potawatomi, and Iroquois people inhabited the region. Dates are difficult to ascertain, but legend, archeology, and solar eclipse history suggest that an Iroquois Confederacy of Five Nations around the Great Lakes formed by then. Those people surely suffered from urological problems and undoubtedly tried many remedies to ease their pains, although the ailments either dissipated or claimed the poor sufferers’ lives. [Above: Painting by Roy Lichtenstein, 1965. Below, Map of Five Nations, De Lisle, 1718. Darlington Collection, University of Pittsburgh.]
French explorers, beginning with Étienne Brûlé, around 1610, Samuel de Champlain, and later René-Robert Cavelier de La Salle, attempted to colonize the regional home of the Cayuga, Mohawk, Oneida, Onondaga, and Seneca who comprised the Iroquois Five Nations. The Tuscarora joined the confederacy in 1722 to become the Six Nations that eventually were overwhelmed by Europeans.
Three.
Prelude to UM. Detroit, a settlement town in the western territory of a young United States, was initially referred to as the straights. Michigan became a distinct territory, carved from the Northwest Territory by congressional act, 30 June 1805. First governor William Hull and presiding judge Augustus B. Woodward described its history, in their first report, with the French penetration of Lake Michigan, the “Ouisconsin” River and the Mississippi down to its “mouth,” defaulting to the French feudal system of property ownership by aristocratic right (seigniorial), but offering no sensitivity to the Native American perspective:
“Prior to this era the settlements of the strait had commenced, and Detroit claims an antiquity of fifteen years superior to the city of Philadelphia. The few titles granted by the government of France were of three French acres in front, on the bank of the river, by forty feet in depth, subject to the feudal and seignoral conditions, which usually accompanied titles in France.” [Michigan Historical Collections. 36:107, 1908.]
The claim in the report refers obliquely to La Salle who buried an engraved plate and cross near what is now Venice, Louisiana, on April 9, 1682 to assert ownership of the territory by France. Hull and Woodward didn’t have all their facts in order regarding Philadelphia, also founded in 1682 but a month earlier on March 4 when William Penn made it the capital of Pennsylvania Colony. Great Britain assumed the French possessions after the 1763 Treaty of Paris ended the Seven Year’s War. Another Treaty of Paris, in 1783, ended the Revolutionary War, and the territory that would become Michigan was acquired from Canada by the United States. The Hull and Woodward Report tells of the sad circumstances of Detroit in June of 1805 just after it had burned to the ground:
“It was the unfortunate fate of the new government to commence its operations in a scene of the deepest public and private calamity. By the conflagration of Detroit, which took place on the morning of the 11th of June, all the buildings of that place, both public and private, were entirely consumed; and the most valuable part of the personal property of the inhabitants was lost. On the arrival of the new government [Woodward arrived Saturday June 29 and Hull on Monday July 1]. A part of the people were found encamped on the public grounds, in the vicinity of the town, and the remainder were dispersed through the neighboring settlements of the country; both on the British and the American side of the boundary… The place which bore the appellation of the town of Detroit was a spot of about 2 acres of ground, completely covered with buildings, and combustible material…” [Central Michigan University. Clarke Historical Library. 1805. Hull.]
Detroit rebounded from the fire and was on the upswing when The War of 1812 broke out and the town, indefensible, surrendered to the British on 6 August. An attempt to regain Detroit by General William Henry Harrison failed in January 1813, but on 10 September Commodore Perry’s fleet of nine small ships defeated six heavily armed Royal Navy ships on Lake Erie and returned the city to the United States. One quarter of the recruited American soldiers were African American. The British retreated up the Thames River in Canada, where the decisive Thames Battle on 5 October turned the tide against Great Britain and Tecumseh’s Confederacy (recounted here in Matula Thoughts last year). This story is a prelude to the University of Michigania, organized in Detroit in 1817.
Four.
New Year resolutions have faded into memory by now for all but the most resolute of us, although it’s worth reflecting that resolutions and intentions reflect the best versions of our imperfect selves. Franklin Delano Roosevelt, an architect of some of the best of modern American society, was particularly good with his public words, few more noteworthy than in his First Inaugural Address on March 4, 1933 during the depth of the Great Depression: “So, first of all, let me assert my firm belief that the only thing we have to fear is fear itself – nameless, unreasoning, unjustified terror which paralyzes needed efforts to convert retreat into advance.” Yet, no more or less imperfect than most of us today, FDR sometimes crumbled from fear himself, as early in WWII with Executive Order 9066 February 19, 1942, authorizing the Secretary of War to prescribe “Military Areas”:
“Whenever he or any designated Commander deems such action necessary or desirable, to prescribe military areas in such places and of such extent as he or the appropriate Military Commander may determine, from which any or all persons may be excluded, and with respect to which, the right of any person to enter, remain in, or leave shall be subject to whatever restrictions the Secretary of War or the appropriate Military Commander may impose in his discretion. The Secretary of War is hereby authorized to provide for residents of any such area who are excluded there from, such transportation, food, shelter, and other accommodations as may be necessary, in the judgment of the Secretary of War or the said Military Commander, and until other arrangements are made, to accomplish the purpose of this order. The designation of military areas in any region or locality shall supersede designations of prohibited and restricted areas by the Attorney General under the Proclamations of December 7 and 8, 1941, and shall supersede the responsibility and authority of the Attorney General under the said Proclamations in respect of such prohibited and restricted areas.” [Below: FDR at Yalta. DG Chandor portrait at SAAM, Washington.]

The Executive Order quickly became actual law on March 21, 1942 when Roosevelt signed Public Law 503, put forth by Congress after 30-minute discussion in the House and an hour in the Senate, thus evicting 122,000 men, women, and children of Japanese ancestry (two thirds were American citizens) from their West Coast homes to incarceration camps. Americans of German and Italian ancestry were similarly targeted, but with much smaller numbers. Another Executive Order, number 9102 signed 18 March 1942, created the War Relocation Authority (WRA) to manage the forced relocation and internment. Milton Eisenhower was its first director, but only for a few months. His successor, Dillon Myer asked Eisenhower if he should take the job and was told:
“Dillon, if you can sleep and still carry on the job my answer would be yes. I can’t sleep and do this job. I had to get out of it.” [NYT 3 May 1965.] [Oral history interview with Dillon S. Myer. Harry S. Truman Presidential Library.]
Ultimately, 18 Civilian Assembly Centers, 10 Relocation Centers of the WRA, 9 Justice Department Centers (with German-American and Italian-American detainees), 3 Citizen Isolation centers (for “problem inmates”), 3 Federal Bureau of Prisons sites (mainly for draft resisters), 18 U.S. Army facilities, and 7 Immigration and Naturalization Services’ facilities were involved in detentions. The Japanese American Memorial to Patriotism During WWII revisits this sad story with the Golden Crane sculpture of Nina Akamu showing two Japanese cranes caught in barbed wire. Semicircular granite walls name the ten main WRA internment camps and The Archipelago on the open perimeter along Louisiana Avenue near D Street in Washington, DC, symbolizes the Japanese Islands and the five generations of Japanese Americans affected by the war. [Below: Two Cranes. DAB January, 2018.]

Five.
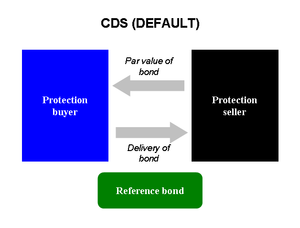
Hourglasses turn the ephemeral notion of time into physical reality. The grains of sand are elementary chemicals assembling by physical rules into worthy objects, stardust like ourselves. Laws of chemistry and physics that created stardust are durable and universal. Human rules are fungible and we hope that representational government and good leaders bend them to fairness, allowing redress when rules are improper, archaic, wrong-headed, or harmful to the public good. All sorts of rules, federal, state, local, professional, organizational, sectarian, familial, and personal ones constrain us, and sometimes they seem to come out of the blue as with presidential directives. Lincoln’s Emancipation Proclamation, considered here last month, and FDR’s Executive Order 9066 raise the issue of these curious sidebars of American law. A report of the Library of Congress, Congressional Research Service, by legislative attorney John Contrubis (updated March 9, 1999) explains the origin and usage of these two “Presidential instruments” (below).

The Constitution provides no explicit authority for executive orders and proclamations, although Article II states: “the executive power shall be vested in a President of the United States,” “the President shall be Commander in Chief of the Army and Navy of the United States,” and “he shall take care that the laws be faithfully executed.” Dogmatic originalism, might then argue to exclude the Air Force from presidential authority, or stipulate that a president execute all laws faithfully to their letter (rather than broad interpretation of Constitutional intent), or that a president must be a “he.” Such pedantic exercises unnaturally infuse human rules with an immutability similar to natural laws of chemistry and physics.

As humans, we elevate some of our laws to higher truths, such as belief in human liberty, the sanctity of life, equality of opportunity, and the right to pursue happiness, recognizing that these “self-evident truths” are perhaps on a higher plane than laws of prohibition, zoning, speed limits, or executive orders. Executive orders are legally binding directives given by the president to federal agencies in the executive branch, while executive proclamations may be ceremonial, policy announcements celebrations (Mother’s Day), or statements of a condition (e.g. of national mourning for the death of George HW Bush). Clearly there is overlap between orders and proclamations; the Emancipation Proclamation was as much an order as a proclamation. [Above: Emancipation Proclamation, Clements Library, University of Michigan. Below: 1914 Proclamation of Woodrow Wilson designating Mother’s Day.]

Six.
Lysekno. Civic laws can cast long shadows that undermine education and science, setting human laws and policies at odds with the natural world. The Trofim Lysekno (1898-1976) story is a cautionary tale. That Russian biologist rejected Mendelian genetics and proposed his own theory of environmentally-acquired inheritance, offering experimental results with improved crop yields by his methods (unverified by others) and convincing Joseph Stalin to embrace Lysenkoism nationally. Soviet scientists who opposed the idea were dismissed from their posts, if not killed as “enemies of the state.” [Fitzpatrick S. Stalin’s Peasants: Resistance and Survival in the Russian Village after Collectivization. Oxford University Press. 1994. p. 4-5.] Forced collectivization and famine followed in the 1930’s, but Lysenko’s political power consolidated and in 1940 he became director of the Institute of Genetics of the USSR Academy of Sciences. In 1948, scientific dissent from Lysenko’s theory was outlawed.
After Stalin died in 1953, Nikita Khrushchev retained Lysenko in his post, but scientific opposition resurfaced and his agricultural influence declined. In 1964, Andrei Sakharov (1921-1989) physicist, architect for the Soviet thermonuclear bomb, but later Soviet dissident and Nobel Peace Prize Recipient (1975), denounced Lysenko to the Russian Academy of Sciences in 1964 saying:
“He is responsible for the shameful backwardness of Soviet biology and of genetics in particular, for the dissemination of pseudo-scientific views, for adventurism, for the degrading of learning, and for the defamation, firing, arrest, even death, of many genuine scientists.” [Norman L, Qing NL, Yuan JL. Biography of Andrei Sakharov, dissent period. The Seevak Website Competition.] [Cohen BM. The descent of Lysenko. The Journal of Heredity. 56:229-233, 1965.] [Cohen BM. The demise of Lysenko. The Journal of Heredity. 68:57, 1977.]
Lysenko died in Moscow in 1976 with only brief mention in the daily national newspaper. His politically enforced scientific pseudo-science had tragic consequences for millions of people in Soviet Russia. Lysenko wasn’t the first to consider the effects of environment on inheritance, Lamarck (1744-1829) had that thought much earlier. Open scientific give and take has since shown that Mendelian and other genetic processes are indeed influenced if not largely regulated by epigenetic factors. Science works well, but not when corrupted by ideology.
Seven.

Too bad Gerrymanders aren’t mythical creatures. These Homo sapiens look-a-likes actually exist, grabbing and abusing transient authority to distort reality and fairness to gain political advantage. Democracy as expressed in our origin-document, The Declaration of Independence is built upon shared belief in fairness, but when fairness is seriously undermined, authoritarianism creeps back into public life – authority of a political party, authority of a leader, authority of a particular ideology, authority of a religion, or authority of a class of people. History shows this human propensity again and again with tribalism, kingdoms, monarchies, dictators, cults, single-party nations, etc. Gerrymander came from Elkanah Tisdale’s cartoon in the Boston Centinel, 1812, showing the district created by the Massachusetts Legislature to favor incumbent Democratic-Republican candidates over the Federalists. [Above: Tisdale’s creature in the Centinel, 1812. Below: Michigan districts.]

Eradication of the gerrymander is one of democracy’s existential necessities. This problem is exacerbated by the algorithmically-targeted misinformation made possible by personal data mining. This perversion of free speech is dramatized in the Netflix film, Brexit.
Eight.

History Hall. Along the passages connecting University Hospital, Frankel Cardiovascular Center, Rogel Cancer Center, and Medical Sciences I buildings are pictures of most of the Medical School graduating classes. Even as faculty and staff walk briskly through them, discussing their work, the decorative walls and the light from the glass tunnel are pleasant and even refreshing. If you have a chance to linger briefly and look, the pictures take your walk through a history of paradigm changes, economic booms and busts, great discoveries, inspiring leaders, wars, bad actors, duds, and all the other stuff of 170 years. Each student and faculty member in the class pictures is an individual summation of countless personal dramas and stories. [Above: David Fox and Joe McCune.]
Maybe stepping aside as chair (I don’t think of it so much as “stepping down” or a loss, but I am truly pleased to have Ganesh Palapattu pick up the challenges, present and ahead) gives me too much time for lingering walks and gratuitous thoughts. Framed by all the larger problems of the world (geopolitical conflict, terrorism, poverty, widening inequality, economic unpredictability, environmental degradation, infectious diseases, and other existential threats) one must wonder: can we humans successfully control our own destiny? If so, some structure and rules are obviously necessary for 7 billion people on a small planet, but will the structures and rules revert to ancient painful models of authoritarian rule and pyramidal hierarchy, or could they tilt toward libertarian, laissez-faire, or anarchistic models although those have never proven successful at large scale?
The question is not merely rhetorical, it is existential and an answer needs to be found between those extremes, within some central range. How we find, set, and reset that optimal place in our laws is the ultimate political question. Representational democracy, even as terribly imperfect as it is, seems to offer the best framework to balance individual freedom and happiness with optimization of societal function, human destiny, and planetary sustainability. This same dilemma of governance, structure, and rule-setting is recapitulated in localities and large organizations, even that of Michigan Medicine. These may seem strange Matula Thoughts for the moment and solutions are beyond the wisdom of this writer, but with 7 billion points of wisdom, good answers should abound. Lingering walks through history halls can help.
Nine.
Academic urology at Michigan effectively began in the autumn of 1919 when Hugh Cabot came to Ann Arbor, and for that reason we begin a year of centennial celebration with our Nesbit Alumni Reunion October 3-5, 2019. Cabot’s 11 years at Michigan were transformative, but disruptive and (yes) often authoritarian, leading the regents to dismiss him in February, 1930, “…in the interests of greater harmony.” His next phase of work was at the Mayo Clinic where he focused on large issues of health care, such as testifying to Congress in favor of multispecialty group practice against the position of the AMA. Cabot’s final book, The Patient’s Dilemma, written in 1940, concludes with reflections on the problems that democratic systems have in planning the future. “It may well be – if we preserve our sense of humor – that we may suspect that the phrases ‘long distance planning’ and the ‘democratic process’ are in fact contradictions of terms.” While allowing for individual freedoms of opinions and rights to change them and exercise them through voting, Cabot explains that a democratic society that cannot make long term plans and carry them out is reduced to an “absurdity.” Cabot ends the book thus:
“…we have an immense body of opinion, part of which is in this country, a handsome part of it elsewhere, which continues in spite of discouragements, to believe that there is in all human beings an inherent and irresistible desire for certain freedoms which can be obtained only under democracy. Such a view seems to me based upon irrefutable evidence going back to the beginnings of the world. Its validity I cannot doubt. Once we admit this premise, once we admit that we believe that there are in democracy certain inherent benefits essential to progressive civilization, then we are driven to the conclusion that though long distance planning under democracy is beset with many vicissitudes, nevertheless such plans must be made and, by dint of good temper and the laws of the cosmos, they may come to fruition.” [Cabot H. The Patient’s Dilemma: The Quest for Medical Security in America. 1940.]
Ten.
Stardust, Hoagy Carmichael’s popular song, came to his mind in 1927 when visiting his alma mater, Indiana University, where he had earned a bachelor’s degree in 1925 and law degree in 1926. Mitchell Parish added lyrics in 1929 and the song has been recorded by Bing Crosby (1931), Nat King Cole (1956), and Willie Nelson (1978) among many others. The music and the lyrics are equally compelling, with Parish linking “the purple dust of twilight time,” the stars, and memories of a lover: “And now my consolation is in the stardust of a song.”
The original title was two words, Star Dust. Astronomers have learned much about the topic since Hoagy’s day: the elements of stardust larger than hydrogen and helium up to the size of iron required solar furnaces for their creation, but larger elements required the greater manufacturing complexity of supernovae. The fact that life is literally made of stardust is not just a figure of speech, the stardust of a song is a lyrical metaphor of a higher order of magnitude. Lying somewhere between cosmic stardust and its human incarnation is the daily work and politics of humanity, and these have been the focus of matulathoughts.org.
I came to Ann Arbor in 1984 from Walter Reed and the U.S. Army at the invitation of Section Head Ed McGuire, who very positively impacted the world of urology and myself. I inherited the stewardship of Michigan Urology from another great urologist and our inaugural chair, Jim Montie. Previous leaders of urology at Michigan educated superb urologists from Nobel Prize winner Charles Huggins and Reed Nesbit, the first section head, through Jack Lapides who trained another splendid cohort, including Hugh Solomon whom we often see at Grand Rounds. [Below, Hugh and Jim.] Following Jack, we had Ed, Joe Oesterling, Bart Grossman, and then Jim. They all brought things to the table, so to speak.

My appreciation is profound to our faculty, staff, Nesbit alumni, and friends of the department. You have made my time as chair a joy. Sandy Heskett has been with me from the start of my administrative duties in Allen Lichter’s dean’s office and she has somehow dissolved the problems of each day and kept our department as well as your old chair on track. Jack Cichon and Malissa Eversole have been incomparable in their work and loyalty to our team. Thanks, too, to my colleagues and friends on the faculty, in the Dean’s office, and on central campus. It has been a great run for me, but it isn’t over yet.
We appreciate your interest and will be back here on the first Friday of March at this website: matulathoughts.org. and meanwhile encourage any comments from you.
David A. Bloom
University of Michigan, Department of Urology, Ann Arbor