
DAB What’s New June 1, 2018
Rules, boundaries, & stories
3722 words
One.

Colors explode as summer opens up in June around Ann Arbor. The visuals are unsurpassed in the UM Nichols Arboretum Peony Garden, adjacent to Mott Children’s Hospital. The garden is a few years short of a century old and derives from Dr. WE Upjohn’s flower collection (pictures above and below, May 29, 2018).

Schools let out in June and summer vacation begins for most students north of the equator, echoing our agrarian history when children needed to be free to work on family farms. Today, farms don’t depend on child labor and most schoolchildren come from urban/suburban homes, the rural: urban ratio having flipped in the last 150 years. In 1870, 25.7% of the US population (38.5 million) was urban and 74.3% was rural, while by 1990 the ratio was 75.2% urban and 24.8% rural (population 248.7 million) and the trend continues, although summer vacation still rules in most schools and workplaces. [Table 4 US Census Data 1993.]

Doctors in training don’t get summers off, they have full 12 month cycles of education, with one random month for vacation, and our new cohort begins its turn next month here in Ann Arbor. [Above: Grand Rounds.] Time has framed graduate medical education in urology since the formalization of the American Board of Urology in 1935. Urology trainees at Michigan spend five years of postgraduate training after medical school, shorter than my time of residency at UCLA, although residents today are increasingly likely to put in additional years for fellowship training. The idea of “duty hour” limitation was a reaction to a few bad training programs that exploited residents, and the 80-hour work week is the national standard for residents in training. Another quantitative constraint is the concept of minimum numbers of specific operative procedures.
A qualitative dimension of regulation, educational milestones, was implemented within the last decade. Milestones reflected the enticing idea that GME should not routinely progress only according to clock, calendar, and case numbers, but according to acquisition of skills. The increased burden of administrative time and paperwork to document milestones, however, has been unmatched by any demonstrable value for trainees or programs and, if common sense prevails, milestones will likely get swapped out for another idea or experiment. Nonetheless, it is clear that time and numbers alone should not be the only measures of residency education.
Our new GME cohort. Residents Kathryn Marchetti from UM, Kyle Johnson from University of South Carolina, Javier Santiago from Baylor Medical School, and Roberto Navarrete from Wake Forest School of Medicine. Fellows Giulia Lane from University of Minnesota (FPMRS) and Jeffrey Tosoian from Johns Hopkins Hospital (SUO). New Faculty: Bryan Sack from Boston Children’s Hospital and Courtney Streur who completes her pediatric urology fellowship both join our Pediatric Urology Division. Kristin Chrouser has joined our faculty this year from the University of Minnesota in NPR and will be mainly at the VA.
Two.
Time, curiously, has no role in baseball, the game of summertime. The sport has no relation to a clock – rather milestones of innings, runs, and outs mark the game’s progress. In this, baseball lends itself to being the ideal summer sport, unfettered by time and limited only by accumulation of three failures or “outs” and innings unless bad weather intervenes or until it gets too dark to play.
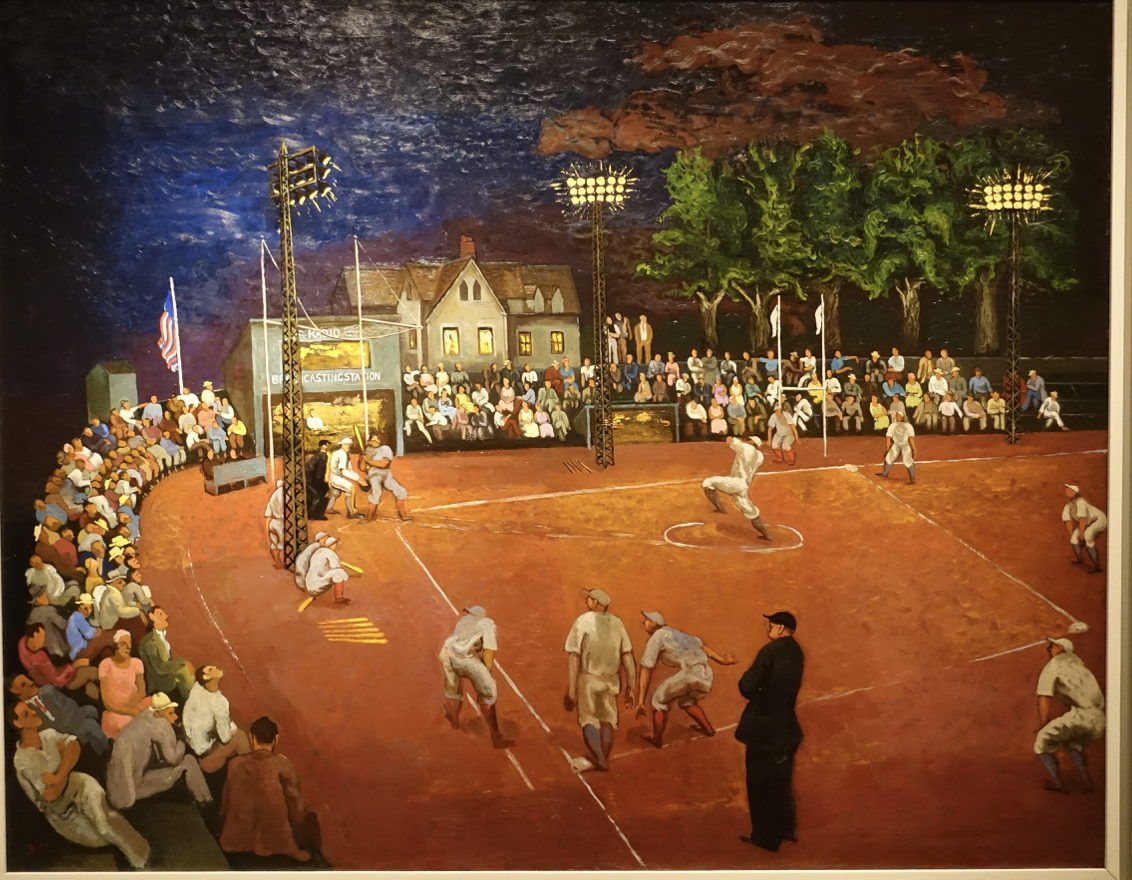
Baseball at Night, a painting by Morris Kantor on display at the Smithsonian American Art Museum in Washington, DC, shows a minor-league game in West Nyack, NY, around 1934. Stadium lighting was a rarity then, given the long days of summer when play could continue until dark, although twilight made the game tenuous. Stadium lights shifted quickly from novelty to necessity and major league teams have played deliberate night games since 1935.
It’s hard to imagine baseball or any other sport without limits and rules, even if arbitrary or parochial, such as the designated hitter rule that now applies to one major league but not another. Rules matter and when different leagues play each other, they find it necessary to have rules that supervene their particular league rules. Rules create fair playing fields, allowing games to go forward and conclude peacefully.
Rules are equally essential for other social activities, organizations, and governments. The USA has the Constitution and Bill of Rights. The State of Michigan has its own constitution and laws, including term limits that guarantee frequent refreshment of the state legislature, but at the expense of deep institutional knowledge of the state and its components. The University of Michigan has its Regent’s Bylaws and Standard Practice Guide, as well as Michigan Medicine’s own sets of Bylaws. In all of these we rely on consensus for decisions, achieved casually in daily operations, more formally in committees (using Robert’s Rules of Order), and more broadly by public voting.
Three.

Communication skills are a pre-requisite for medical practice in both the essential transactions of direct patient care and in the complex team play of modern specialty medicine. [Above in foreground, Brent Williams, Professor of Internal Medicine, communicating with Michael Giacalone, Jr., Chief Medical Officer of the Hamilton Community Health Network in Flint.] Listening, speaking, reading, and writing skills are taught with variable degrees of success in elementary schools up through college, but medical practice demands more vocabulary and capabilities. Medical students, it is said, double the size of their vocabularies.
The traditional algorithm of healthcare starts with listening to the concerns of patients and then probing for additional information to construct a medical history, including relevant comorbidities and circumstances. Patients are physically examined and data is assembled into coherent narratives. Diagnosis, prognosis, and therapy derive from those stories in which authenticity and accuracy are assumed.
Modern electronic systems impose new communication challenges. Email and texting are immediate and convenient, but lack the human factors of facial cues, thoughtfulness, and social grace. Electronic medical records (EMRs) constrain work flows to templates and replace human narratives with check lists, pop-up choices, keyboard entries, and cut-and-paste phrases. The actions of data entry detract from listening, looking, and communicating with patients. Healthcare processes today do not prioritize stories, and it seems to me that appreciation of the art of the story lies at the heart of excellent clinical care. It’s no great leap of faith to claim that the art of authentic storytelling and story construction is the basis of most human relations, from compelling stories around campfires to A3 storytelling in lean process engineering. Truth and authenticity matter. Listening to them and weaving them are art forms.
Four.
Physician-author William Carlos Williams appeared on these pages earlier this spring and since then I’ve been thinking of the different contexts in which physicians write, and first and foremost, physicians write the stories of their patients.
Williams, you may recall, was the author of Spring and All of which a recent edition included an introduction by C. D. Wright comparing Williams to an earlier poet from New Jersey, Walt Whitman: “Like Whitman, he [Williams] would gradually come to a great human understanding, an apprehension that eluded most of his peers.” [Spring and All. WC Williams. New Directions Book, 2011.]
We pursue that greater human understanding on a daily basis, working in medicine, through stories learned and experiences gained, patient-by-patient. The dilemmas of patients are understood in terms of their stories, that must be heard, elucidated, and constructed from evidence and reasoning on the part of those who undertake the responsibility for helping. Stories are important to people, and we dignify them with our attention.
Electronic medical records are poor platforms for authentic narratives. The construction of narratives in the minds of physicians and the translation to visible words in some medium is a core element of the profession of medicine, framing the response of the care-giver in terms of advice, reassurance, therapy, and prognosis. This is the central organizing feature of the doctor-patient relationship, comprising the daily shop-talk of medical practice. A story must be accurate, with true facts, but also authentic, in reflecting circumstances and co-morbidities (an economist might call these externalities) framing the “present illness” and creating a context for further conversation and therapy. In my experience, an authentic and empathetic story only fully emerges after the history, physical exam, and further discussion with patient and family.
My own clinic notes were once written or dictated well-after the clinical visit when the story was relatively complete and coherent. The reduction of clinical notes to formulaic elements such as the SOAP format (subjective, objective, assessment, and plan) or the E&M format (Evaluation & Management: chief complaint, history of present illness, review of systems, etc.) fits computer entry systems nicely, but has disrupted the traditional medical work-flow that create stories.
It is challenging to find the words to describe this fundamental type of medical writing whether in narratives or EHR. Quotidian medical communication seems to fit, even though not everyone is familiar with the use of quotidian for daily or routine. Quotidian communication must be accurate, truthful, and authentic to each patient. Most healthcare workers are writers and their products are stories of patients. A brief piece in The Lancet by Roger Kneebone called “The art of conversation” expresses the idea of the clinical conversation that we have clumsily called “taking a history.” Kneebone expressed his thoughts more elegantly than I have, so I’ll just quote two sentences and refer you to the rest. [The Lancet. 391:731, 2018.]
“A conversation is a one-off live performance that can never be repeated. Its essence is its evanescence, and attempts to capture in writing are as thin as reading the script of a play or film.”
Five.
Stories suffuse all types of medical writing. Scientific writing for journals, grants, or textbooks is the bedrock of healthcare research and progress. Just as with stories of patients, this writing is predicated on accuracy, and clarity is enhanced when a meaningful story is constructed from the science. Medical journalism, another form of medical writing, communicates to the public about medical science and practice. Medical memoir is another important genre, also written for the public but usually as personal storytelling or essays.
William Carlos Williams and others divert into creative reflections through prose and poetry. These writers mainly tell stories they create, often based on authentic experiences, but with “literary license.” Many of these physician-writers venture into fiction at the other end of the spectrum of medical writing, although this too requires authenticity in that stories revolve around individual experiences, conflicts, tensions, issues, and environments that are genuine to the reader’s senses. The fictions may involve other species or galaxies, as with the work of Michael Crichton, but if the stories are well-crafted they contribute to that greater authentic human understanding. To summarize medical writing variants: a.) the daily writing of clinical practice, b.) scientific writing, c.) medical journalism, d.) medical memoir, e.) creative reflections, and f.) fiction.
We are a species of stories and understand ourselves through stories far better than through data. That greater human understanding is accessed through narrative better than through numbers. The novelist Kazuo Ishiguro, in his 2017 Nobel Prize Lecture, praised the “… quiet private sparks of revelation …” to be found in stories. “Stories can entertain, sometimes teach or argue a point. But for me the essential thing is that they communicate feelings. That they appeal to what we share as human beings across our borders and divides.” [Ishiguro. My Twentieth Century Evening and Other Small Breakthroughs. AE Knopf. NY 2017.]
Six.
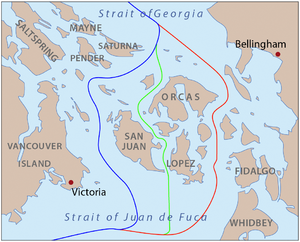
A pig story. It doesn’t take much to disturb a comfortable status quo or otherwise disrupt peaceful human relations. An obscure story exemplifying this began on June 15, 1859 on San Juan Island, a place east of Vancouver Island where both the United States and Great Britain claimed sovereignty, after the Oregon Treaty of June 15, 1846, exactly 13 years earlier. [Below: blue Haro Strait boundary favored by US, red Rosario Strait favored by Britain, green compromise proposal. Copyright Derek Hayes, Historical Atlas of the Pacific Northwest. Sasquatch Books, Seattle, 1999.]
Peaceful co-existence remained in play until a British pig, owned by Hudson’s Bay Company employee Charles Griffin, wandered onto an American farm to eat some potatoes. This wasn’t the first transgression and Lyman Cutlar, the American farmer, shot and killed the trespassing pig. Cutler’s offer of $10 compensation was refused and the British threatened to arrest him. Sixty-six American soldiers under the command of Captain George Pickett were dispatched to the island to prevent British forces from landing. The British countered, bringing three warships offshore, soon escalating to five ships, 70 guns, and 2140 men. American forces then swelled to 461 men with 14 cannons, as diplomacy failed and the dispute escalated into The Pig War. The British governor of Vancouver Island ordered Rear Admiral Robert Baynes to land his marines on San Juan Island, but Baynes wisely refused to further escalate the “squabble over a pig” and the war remained bloodless, aside from the porcine tragedy.
In October, President Buchanan sent General Winfield Scott to resolve the crisis and negotiations resulted in an agreement that the British could occupy the north half and the Americans the south with each side allowed up to 100 troops pending further formal agreement. No wall was built, and in 1872, a full 13 years after the ill-fated pig, an international commission led by Kaiser Wilhelm I, decided that the entire island should fall under American control and so it remains.
Seven.
Henry Martyn Robert was one of the 66 American soldiers stationed on San Juan Island under Pickett’s leadership. It’s hard to know how he felt about his mortal jeopardy over the cause of a pig, but it’s a good thing the conflict remained bloodless and Robert went on to bigger things. Born in Robertville, South Carolina, he grew up in Ohio where his family moved due to their opposition to slavery. Robert’s father, Reverend Joseph Thomas Robert, would later become the first president of Morehouse College (1871-1884). Henry went to West Point and graduated fourth in his class in 1857, becoming a military engineer and building the fortifications on San Juan Island in 1859. He remained with the North during the Civil War, attending to defenses around Washington, Philadelphia, and New England Harbors. After the war, he served the Army Division of the Pacific from 1867-1871, then developed ports in Wisconsin and Michigan, later improved harbors in New York and Philadelphia, constructed locks and dams in Tennessee, and performed more civil engineering pertaining to the Mississippi River and Hurricane Isaac in Galveston. He died in 1923 and is buried at Arlington. [Below: Brigadier General Henry Martyn Robert, Wikipedia.]

Although Robert’s military service was significant, we remember him today for his civil engineering of practical rules for human interaction. These came about in 1876 after losing control of a church meeting he was leading in New Bedford, Massachusetts when it erupted over abolitionist views. Robert blamed his ineptitude for the fiasco and decided to teach himself how to run a meeting. His study of the procedures of the House of Representatives led to his Pocket Manual of Rules of Order for Deliberative Assemblies. He wrote:
“One can scarcely have had much experience in deliberative meetings of Christians without realizing that the best of men, having wills of their own, are liable to attempt to carry out their own views without paying sufficient respect to the rights of their opponents.”
Robert’s world was framed by his gender and faith, but his rules have endured because they are independent of his particularities. Robert’s Rules of Order apply to almost any human gathering and, like the rules of baseball, Robert’s Rules level the playing field and allow the game to go forward. [“Historical Vignette 038 – An Army Engineer Brought Order to Church Meetings.” U.S. Army Corps of Engineers – Office of History. November 2001. Retrieved 2015-12-02.] His rules offer protocols for civilized and democratic behavior.
Eight.

Michigan hosted its first Teeter Symposium last month, focusing on bladder cancer in honor of our Ann Arbor friend Bob Teeter, who died a decade ago from bladder cancer in spite of radical cystectomy. [Above, Bob and Betsy Teeter; below, Teeter Laboratory Plaque.]

Since then, knowledge and therapy of bladder cancer have increased by a quantum leap, although more leaps are necessary to obliterate the pain, suffering, and mortality of that disease. The day-long event, organized by Alon Weizer, featured 2 guest speakers and held an attentive audience that topped 50, with excellent talks and superb discussions. The event fulfills one of the items on my bucket list as department chair and honored not just Bob and his surgeon Jim Montie, but also some generous gifts for laboratory investigation that we gained after Bob passed away.

The first guest lecturer, Thomas Bender, MD, PhD (above) from Dow Chemical, spoke about the Health Hazard Evaluation Program for former employees of a chemical plant that had been closed in 2002, but Dow later acquired its parent company, Morton, in 2009. As I sat in the audience, wondering how to link this month’s Matula Thoughts to the Teeter Symposium, Dr. Bender said a magic word: Paterson. That’s where the chemical plant had been since 1929. Paterson, New Jersey, was the home of William Carlos Williams.

The next invited speaker, Elizabeth Plimack MD, MS, Chief of Genitourinary Medical Oncology at Fox Chase Cancer Center, grew up in Ann Arbor. Her parents and mentor Richard Swartz were on hand to hear her excellent talk Immunotherapy and Beyond. In attendance was Monica Liebert (Nesbit 1984 below), now retired, but still working in our laboratories. Monica developed many bladder cancer cell lines in her heyday and these are still utilized in our research efforts.

Our own Khaled Hafez (below, Nesbit 2004) closed the event with a superb talk on Clinical Management of Patients with Locally Advanced Bladder Cancer, a topic close to his heart and emblematic of his skill set, as he is surely one of the best in the world at this craft.

Nine.
The AUA annual meeting last month in San Francisco featured the usual strong Michigan presence. San Francisco was also the site in 2010 where the picture of our inaugural chair, Jim Montie (Faculty Nesbit 1995), was taken. In addition to turning over a very strong group of faculty and department, in 2007 when the current departmental administration began, Jim turned over a positive team culture, rather than a “me-me-me” culture. Jim not only remained relevant to the department, but remains a keen participant and a role model of leadership.

Looking through those 2010 Nesbit reception pictures, I found a picture of the late and truly great Cornell Urology Chair, Darracott Vaughan, flanked by Jennifer Anger of UCLA and Hunter Wessells, chair at the University of Washington in Seattle (below).

But now back to 2018.

Above: Emilie Johnson, Nesbit 2011, with her iconic mentor from Boston, Alan Retik. Below: Julian Wan, Nesbit 1990, at one of his podium appearances, knocking it out of the park.

[Below: Music reception with Khurshid Ghani, Faculty Nesbit 2013, & David Miller, Nesbit 2005.]

The Nesbit reception this year at the Hotel Vitale on Mission Street hosted around 100 alumni, friends, and current team of the Urology Department. Below, a partial view of the crowd.


[Above: Damon Davis, Nesbit 2007. Brian Sack will start with us in pediatric urology this summer. Kristin Chrouser joined us this winter from Minneapolis and is centered at the VA. Below: Irene Crescenze current fellow FPMRS, Cheryl Lee, Nesbit 1997, now chair at Ohio State, Bert Chen, Nesbit 2006.]


[Above: Stu Wolf, Faculty Nesbit 1996, now in Austin, Udit Singhal PGY 2, Alon Weizer Faculty Nesbit 2005, Bunmi Olapade-Olaopa Nesbit, 2000. Below; Betty Newsom, Nesbit 1990, Bart and Amy Grossman, Nesbit 1977.


[Above: Lynda Ng, Nesbit 2005 and Jerilyn Latini, Faculty Nesbit 2003. Below: Steve & Faith Brown, friends of Michigan.]


[Above: Tom Stringer, Dept Urology Florida, Barry Kogan, Nesbit 1981 and Chair Albany. Below: Hugh Flood, Nesbit 1991, of Clonlara, County Clare, Ireland. Below: Simpa Salami, Nesbit 2017 & guest Mohamed Jalloh of Dakar, Senegal.]

Ten.
Boundary matters. A few months past the JAMA column, A Piece of My Mind, came from Jeffrey Milstein at Penn Medicine [Milstein. The envelope. JAMA. 319:23, 2018] and detailed his office visit with a 70-year-old patient who carried a large white envelope, assumed to be “outside records.” Most of us get these, not infrequently, indicating that a second or third opinion is expected. On the occasion of this particular visit, the details were those of a 32-year old son who had recently passed away due to cancer. The envelope contained a stack of records with an obituary on top. The patient first wanted to talk about his son and then the course of his disease, tests, hospitalizations, treatments, and emotional toll. Then, after “a long moment of silence” the patient explained that he himself had not been to a physician in years, but needed to tell his son’s story before committing to his own care. The clock had run down by then and “the time for the visit” was over leaving nothing that could be documented in the EHR about the patient himself. The author noted “so another visit must be scheduled.”
So, it seems medical care today has tight boundaries of time and information. Boundaries for nations, sports, politics, education, business, are important, but some are more important than others. The Pig War, a foolish dispute, easily could have escalated to bloodshed, leaving us no Robert’s Rules. Rules and boundaries in sports allow games to proceed fairly and end peacefully. Some boundaries in health care are tight and timeless, as evidenced in the Hippocratic Oath or as shamefully dishonored by occasional bad actors. The constraints of the EHR are self-inflicted wounds of the business of medicine, and should be viewed with minor contempt and never honored at the expense of a patient.
Baseball, timeless as it is, nonetheless must be somewhat mindful of the clock. Some fans may have babysitters, while transportation drivers and other workers are paid by the hour. The number of pitches thrown is a clock of a sort. Still, the essence of the game is indifferent to time. The same is true for conversations with patients. Life and schedules are much easier when each patient’s visit goes according to clockwork precision, but the essential transaction of the crucial conversations not infrequently runs afoul of anticipated timed encounters. These conversations are unique in the human repertoire and can have the most profound implications. Skilled clinicians know when and how to diplomatically crowd the later patients, run through lunch, or regroup with an expansive patient later in the day or soon thereafter. Such is the art of medicine.
Thanks for reading Matula Thoughts this June, 2018.
David A. Bloom
University of Michigan, Department of Urology, Ann Arbor
