
Matula Thoughts Sept 1, 2017
3866 words
Dancers & Michigan’s third century
One.
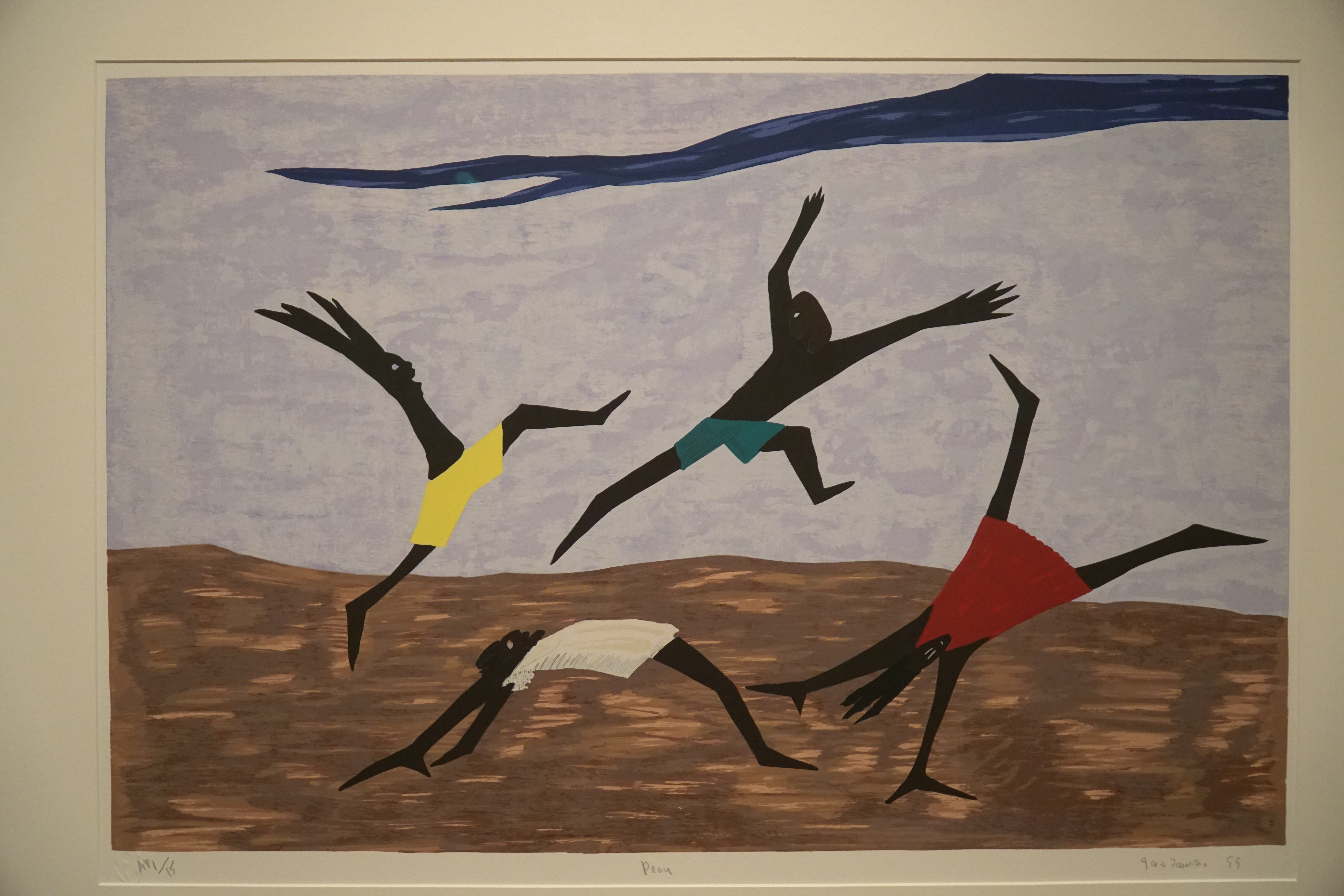
Summertime play draws to an end and work comes into sharper focus this September, as the University of Michigan enters its third century. Medical education’s academic season has been well underway for 2 months as now the rest of the University of Michigan comes back on line and takes up the challenge of examining the world anew. Autumn academic meetings lie ahead and our faculty become traveling salesmen for their ideas. History has shown that many big ideas in urology have come from Michigan and we anticipate many more are ahead. Nesbit urology alumni will reconvene in Ann Arbor this month for a scientific meeting and see the Air Force Academy play Michigan in football. [Above: Jacob Lawrence. Play, 1999. © 2017 The Jacob and Gwendolyn Knight Lawrence Foundation, Seattle / Artists Rights Society (ARS), New York]
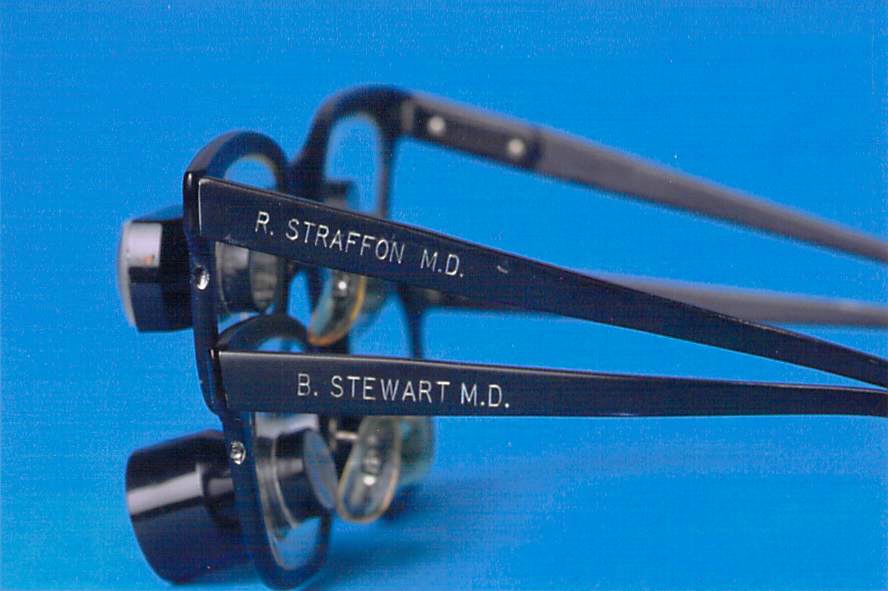
Individual views of the world are shaped by one’s lenses and frames, literally and figuratively. Bob Uzzo, our Nesbit visiting professor this month, once sent me a picture of surgical loupes belonging to legendary Michigan Urology alumni, Ralph Straffon and Bruce Stewart, who had brilliant careers at the Cleveland Clinic. Crisp block letters identify the owners so we know who owned each one, but can only guess how the world looked to either of them. These two remarkable Nesbit trainees impacted hundreds of thousands of patients, thousands of students, and hundreds of trainees. They added to the progress of urology worldwide and both men cherished their Michigan origins and wore their Block M’s proudly. I was lucky to have known Ralph, but never met Bruce. Their photographs hang on the wall outside my office [Above glasses; below Ralph in center, Bruce upper left]. David Miller profiled Ralph for the Bulletin of the American College of Surgeons. [Miller DC, Resnick MI: Ralph A. Straffon, MD, FACS, 1928-2004, remembered. Bull Am Coll Surg 89:32, 2004.]

Two.

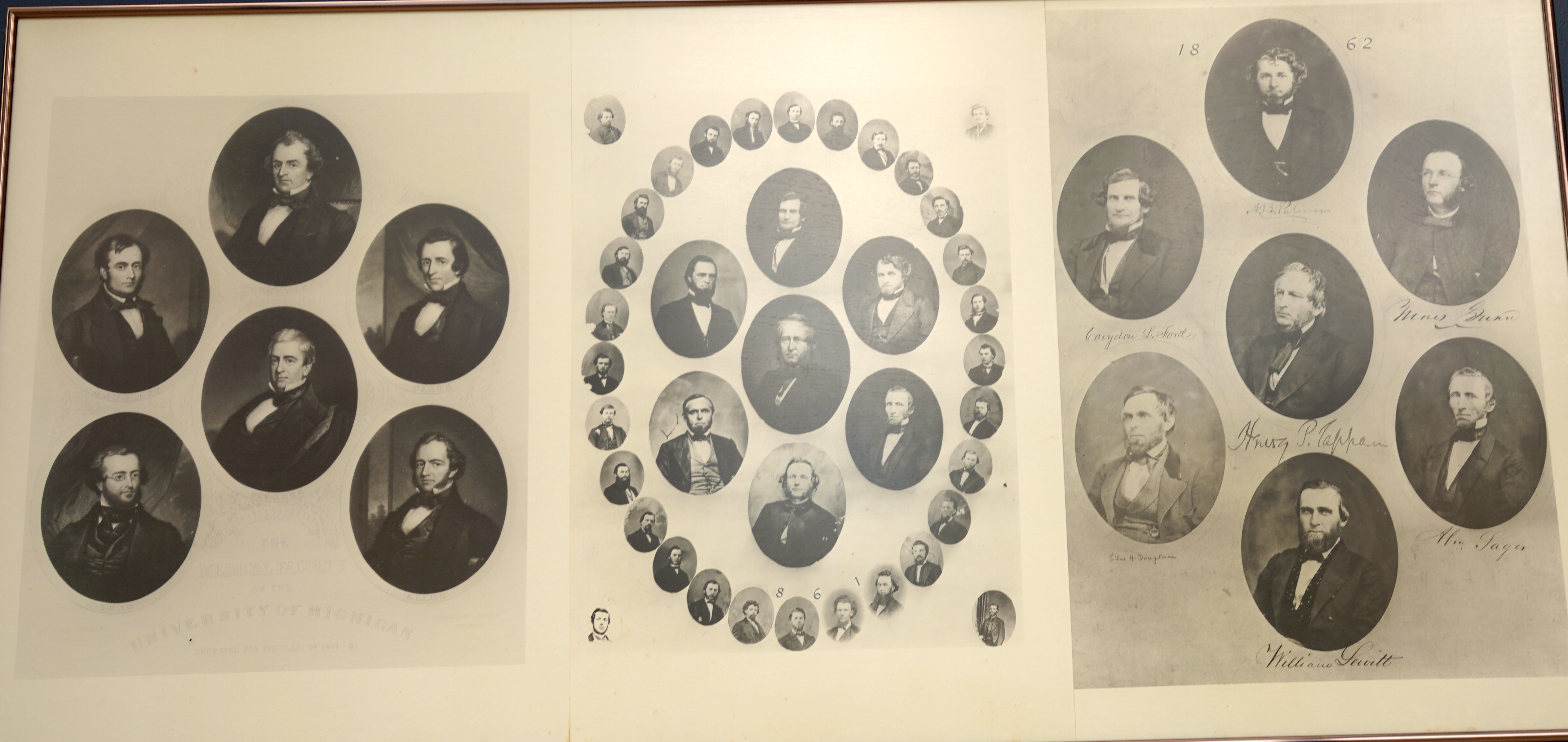
Block M’s. Pictures on our walls bring the past into focus on a daily basis and as you walk from the Main Hospital to the Cancer Center you can see the Block M on the Medical School diplomas, first as a font and later as a symbol. The class of 1861 (below) is the first in the lineup. No pictures of previous classes, going back to our origin in 1850, seem to exist. (A fire in 1911 destroyed the Medical School building with some of the original early pictures.) In 1864 an M-font vaguely resembling a block M is evident in the word “Michigan.” The first typical Block M (with serifs) appears in letters in the picture title, Departments of Medicine and Surgery in 1881. This occurs again in the text of 1883 and 1884, but is gone in 1885. Note that 1883 has 2 class pictures, the additional one being an informal one with the entire class sitting together. That additional picture was given by 1883 class member W.F. Mills to classmate William Mayo years later, in 1936.
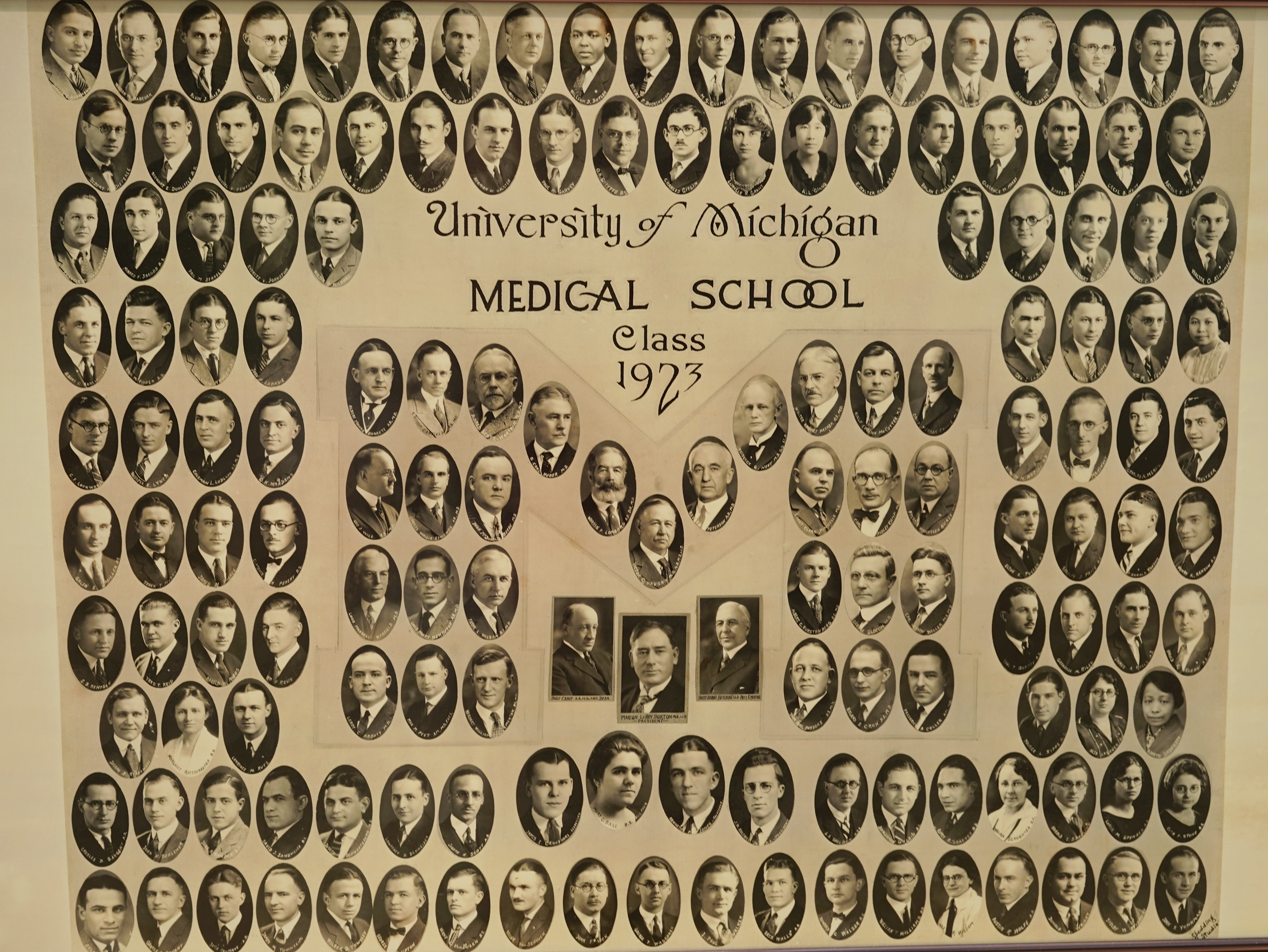
The Block M became a deliberate symbol or logo in the Medical School 1923 class picture, with 29 faculty portraits contained within an M outline (below). Three other faculty (President Burton, Emeritus President Hutchins, and Hugh Cabot who was simultaneously dean, chief of surgery, and solitary urologist) share space outside the M shape and under the center.
The Block M tracing features faint extensions at the bottoms of the letter, called serifs, with squared edges as “blockish” as the M itself. Additional “side” serifs adorn the top outside portions of the vertical limbs of the letter. This style of serif is called a square or slab serif and it continued in subsequent class pictures, although 1928 and 1929 offered oblique views of the Block M. The frontal view was restored in 1930, the year Cabot was fired by the regents (February 11). The 1931 picture was significant for urology including both Cabot and his former trainee Reed Nesbit, the sudden head of urology. Curiously, Cabot’s picture remained even in the 1932 picture. His firing left the Medical School without a dean until 1935 when Albert Furstenberg was appointed. Block M with serifs continued through 1944, although with minor variations including one oblique reversion in 1935. Two 1943 class pictures feature separate classes, reflecting the intensified medical education during the war effort. The 1945 Block M has short and thin slab serifs.
Three.
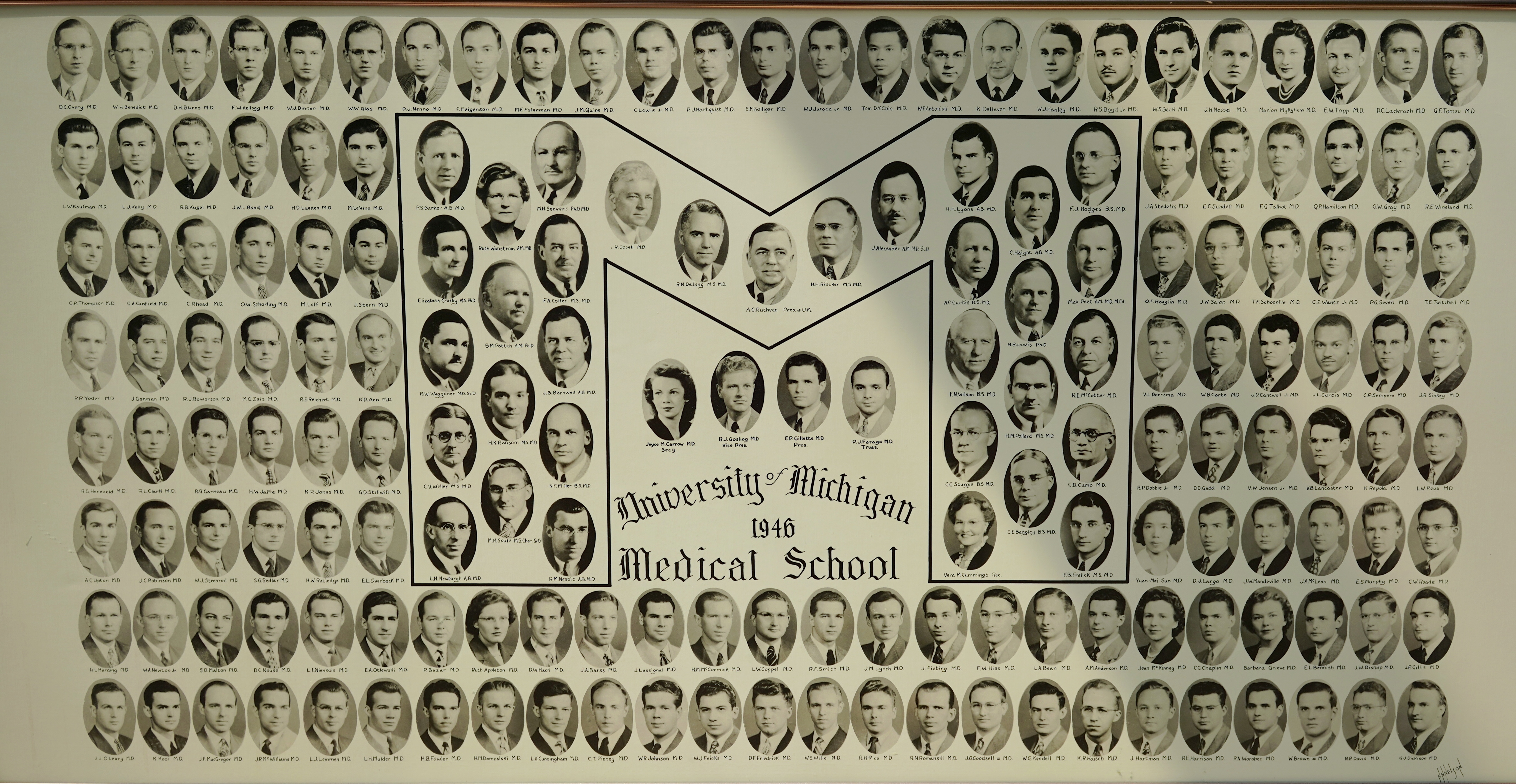
A 22-year run of Block M’s with serifs ended in 1946 when the shape simplified to a simple, unadorned Block M outline, sans serifs, containing 33 faculty including Nesbit within the logo.
No 1947 picture is present on the wall. A Block M with serifs returns in 1948. The 1949 picture has no Block M insignia, font, or outline whatsoever. Dean Furstenberg is present and the faculty include Nesbit now with some gray hair. A variant Block M with serifs is present in 1950 and 1951, and now the dean’s name is spelled “Furstenburg.” A sans-serif Block M outline reappears in 1952 including Nesbit again. The traditional Block M outline with serifs is restored in 1953, 1954 (the dean is back to Furstenberg), and 1955. The UMMS lists Albert Carl Furstenberg as dean 1935-59, so the variable spelling is odd. Interestingly, from the urology perspective, junior faculty member Bill Baum, is present in 1953 and again in 1954 then with Jack Lapides. Narrow and tall serifs adorn the Block M outline in 1956 with “Furstenburg” again, but the 1957 picture oscillates back to a sans-serif Block M with Furstenberg and faculty again in the M-shape outline. Serifs returned in 1958. Lapides represented the Section of Urology on his own in 1957 and 1958.
The Block M outline vanished in 1959, replaced by a small filled-in Block M logo over the year. This unusual picture shows no faculty except for President Hatcher and Dean Furstenberg among the medical students. The 1960 picture has a sans-serif Block M symbol, but as in the previous year no pictures within the logo. Nesbit returned that year among 26 faculty shown with the class, plus the university president, Dean Furstenberg, emeritus dean, 2 assistant deans, and one administrator. A solid filled-in black Block M logo is present in 1961, but the picture contains no faculty. Redundantly, that year, the class officer pictures show those students a second time. The same format repeats in 1962. Faculty return to the picture in 1963 but only 42 (presumably only senior ones) plus a non-faculty administrator within a Block M sans-serif, that repeats in 1964 with faulty including Nesbit. That pattern persists in 1965 with 27 faculty including 2 “class mentors” and some chairs. Also present are President Hatcher, the hospital administrator, and an assistant administrator. Nesbit is missing again.
Since 1966 each picture features a fairly typical Block M outline with slab serifs and faculty embedded the letter. Nesbit was back in ’66 but looks older and returns in 1967 for his last picture, gone finally in 1968, the year of his retirement. Lapides appears as section head of urology in 1969, but isn’t pictured again. The picture format has remained relatively stable since then, although as faculty grew to over 2500 by now, general faculty pictures were replaced by dean’s office faculty and chairs.
With the recent expansion of Michigan Medicine’s footprint and regional affiliations the Block M has undergone tweaking and constraints, reportedly to maximize its effect. Articles in the Michigan Daily by Austen Hufford (October 20, 2014) and Tim Cohn (March 28, 2017) explain the evolution of the maize-colored Block M from an 1888 football team photo and 1891 team uniforms to its present proxy for the larger University of Michigan. Michigan’s branding blossomed under athletic director Don Canham, as reported by the late great sports writer Frank Deford in Sports Illustrated in 1975. [Deford. No death for a salesman. Sports Illustrated. July 28, 1975]
![]()
[Above: instructions on use of the University of Michigan logo]
Four.

West Shore Urology. The Block M will extend to Muskegon and the West Shore Urology (WSU) practice this fall. Started in 1972 by Thomas Stone (retired in 2000) the practice now consists of Kevin Stone (son of Thomas), Joe Salisz, Jennifer Phelps, Brian Stork, and Adam Walker (in Alaska at the time of picture) who join us as Clinical Assistant Professors of Urology as their practice becomes a UM ambulatory care unit. WSU is a high-level practice with philosophical commonalities to UM and strong ties, particularly through the Michigan Urological Surgical Improvement Collaborative (MUSIC) run by David Miller and now Khurshid Ghani. We will learn how to collaborate at a significant distance. Lisa Thurman is the PA at WSU.
Joe, Brian, and Kevin trained at Beaumont, and Jessica at Henry Ford, institutions populated by Nesbit alumni including Ananias Diokno, Jay Hollander, Evan Kass, and Hans Stricker. Adam Walker trained with Nesbit alumnus Barry Kogan at Albany Medical Center. Adam, a Hillsdale College and University of Minnesota Medical School graduate, comes from Elmendorf-Richardson Joint Base in Alaska where he was Chief of Urology, a position formerly held by our Nesbit alumnus David Bomalaski. Dave, by the way, remains in practice in Anchorage as the only pediatric urologist in the state and in the entire Indian Health Services system. The WSU team staffs Hackley Hospital, Mercy General Health Partners, Gerber Hospital in Fremont, North Ottawa Community Hospital, and Muskegon Surgical Center. Their diverse skills and perspectives will enlarge our Department.
Five.

American artist Jacob Lawrence (1917-2000) was born 100 years ago (September 7). I first saw his work at the Phillips Collection in Washington, DC when in town for a meeting of the American Academy of Pediatrics Section on Urology. His 60-panel Migration Series, funded by the Works Progress Administration and completed in 1941, illustrated the story of the Great African-American Migration from the rural south to the urban north, beginning around 1910. Lawrence worked on the paintings more or less simultaneously to maintain a uniform stylistic sense, he called “dynamic cubism” and considered the work a unity rather than 60 individual paintings.
Fortune Magazine in 1941 published 26 paintings from the series. Ironically, the paintings are now divided between the Phillips Collection (odd-numbered), where I first saw Lawrence’s work, and the Museum of Modern Art in New York (even-numbered). In 2015 and 2016 the split collections were merged and exhibited as a complete set at each museum before returning to their previous homes. Three-dimensional reconstructions of this work form the introduction to the current Kathryn Bigelow film, Detroit. Lawrence told other stories in collections of paintings featuring Harriet Tubman, Frederick Douglass, John Brown, Toussaint L’Ouverture, and a set called The Builders Series.
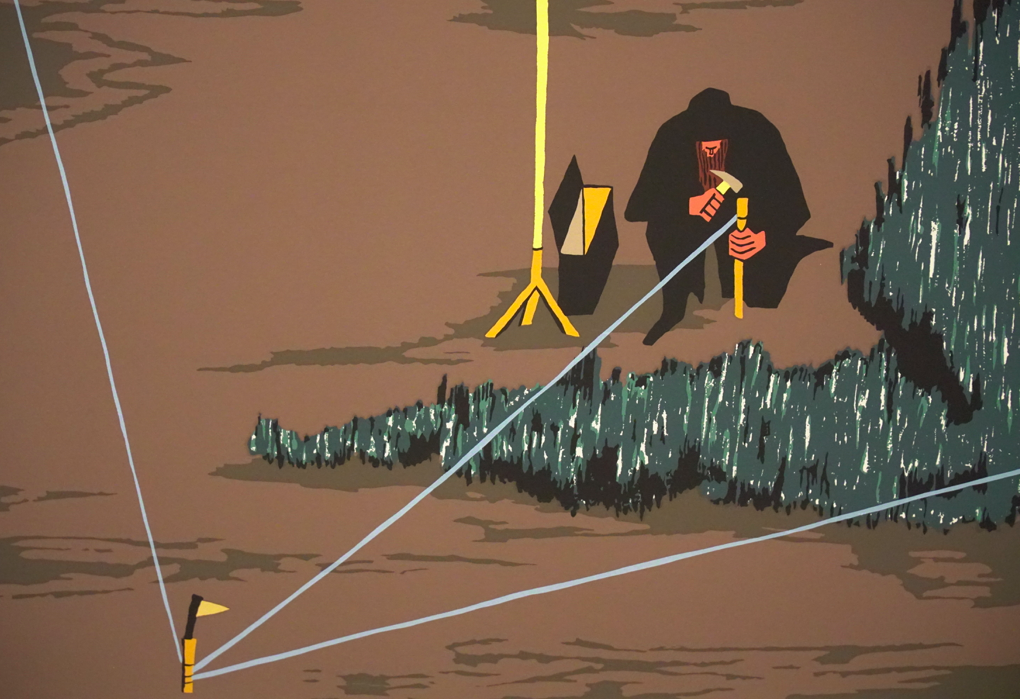
[Photograph above: Jacob Lawrence, Peter A. Juley & Son Collection, Smithsonian American Art Museum J0001840. Original photograph by Geoffery Clements. Image courtesy of the American Federation of Arts records, 1895-1993 in the Archives of American Art, Smithsonian Institution. Below: John Brown as surveyor in The John Brown Series. © The Jacob and Gwendolyn Knight Lawrence Foundation]
Six.
Throughout most of human history health care was delivered by single individuals. Presumably starting out in clans and villages our predecessors in healthcare accumulated healing skills through practice of their arts. Midwives, shamen, herbalists, and the stone doctors mentioned by Hippocrates, specialized in skills. By mid-16th century specialists such as internists, barber-surgeons, and apothecaries were assembling in guilds. Subspecialization reached full display in mid-20th century, when most physicians sought special knowledge and skills based on organ systems, technologies, age groups, or sites of service such as emergency departments and ICUs. The career-defining piece of medical education shifted from medical schools to graduate medical education (residency training) now involving over 100 areas of focused practice, often taking as much time or more than medical school years. The downside of this plethora of specialties is a complex clinical terrain in which patients shuffle among specialists, responsibility is diffuse, hand-offs incur errors, patient satisfaction sinks, and costs soar.
It is natural that arborization of medical skills is countered by nostalgia for omnipotent physicians to take complete care of patients or at least “quarterback” the specialists. This notion of primary care vs. specialty care, however, is more a political distinction than an epistemological one. The idea that everyone should have a “primary” caregiver who will identify specific needs for “specialty care” in patients and make proper referrals (administratively approved by third parties) is attractive, but the reality is that many, if not most, patients needing something specific, identify that need themselves – broken bones, eye trouble, urinary infection, chest pain, etc. – and find care through an emergency department or direct referral to specialists. The modern dilemma of coordinating health care teams, epistemologies, funding mechanisms, education, research, public policies, markets, while maintaining equity is acute. This is the arena of health services research.

Our Dow Health Services Research Symposium is in a bye year, and will hold its 4th meeting in 2018, highlighting our best faculty and resident work and bringing notable young urologists from across the country to similarly showcase their academic wares. Above you see last year’s symposium where Chad Ellimoottil, Michigan Urology Assistant Professor, highlighted Avedis Donabedian, Michigan’s great founder of health services. I first heard Donabedian’s name through Jim Montie and David Miller who gave me the classic 1966 paper. [see Berwick and Fox, Milbank Quarterly 94: 237, 2016] Health service researchers frame clinical problems one way, urologists view them another way, patients have personal points of view, and family members have their own perspectives. All those visions matter, although that of the patient usually dominates for it is on the patient’s behalf that society marshals the resources of treatment.
Seven.
Responding to thoughts on secularism and sectarianism in these pages last month, my friend David Featherman – Professor Emeritus of Sociology, Psychology, and Population Studies and former Director of Michigan’s Institute for Social Research – took my comments to a deeper and more significant level, writing:
“Of course, the most common antonym of secular is sacred, although partisan or sectarian appear in some thesaurus sources, as you note. As a general mental puzzle for me these days I wonder if our secular society, for all its other benefits you note, has verged, in some instances or quarters into sectarianism – in the sense of illiberal, intolerant and perhaps even partisan … Certainly, what I point to is not religious sectarianism, although one might admit to a quasi-religious sectarianism …
Those docs-to-be [referring to the White Coat Ceremony], touching patients with their stethoscopes, strike me as potentially moving beyond the non-spiritual or secular into a realm of human interaction not entirely bound by rationality and reason or lacking in the stuff of human compassion or failing to acknowledge something like a ‘mystery’ in life and death … What strikes me as I write is that the white coat might symbolize one of the larger dilemmas of our time, namely, how to draw upon the sacred and the secular as complementary resources …
If zealots … only can see opposition, in archly incommensurate terms, we shall fail to build that cosmopolitan, tolerant but at the same time spiritually, morally, and ethically grounded world. Without the latter resources, an exclusively secular world of wholly liberated individuals can easily lose its bearings to entropy. Those young docs in training have extraordinary opportunity to teach us how to achieve a more complementary cosmopolitanism, day by day, patient by patient.”
David’s point, in a nutshell, seems to be that we cannot isolate secular professionalism of health care from a notion of the sacredness of human life and morality. This veneration transcends specific religions, deities, or other schools of belief, but it is a sacredness that the secular world needs to contain, even if this seems somewhat paradoxical. Lacking this, Professor Featherman rightly professes, a secular society and its cosmopolitan world of nations, religions, markets, universities, politics, and corporations, spin out centrifugally and dissolve into entropy.
Eight.
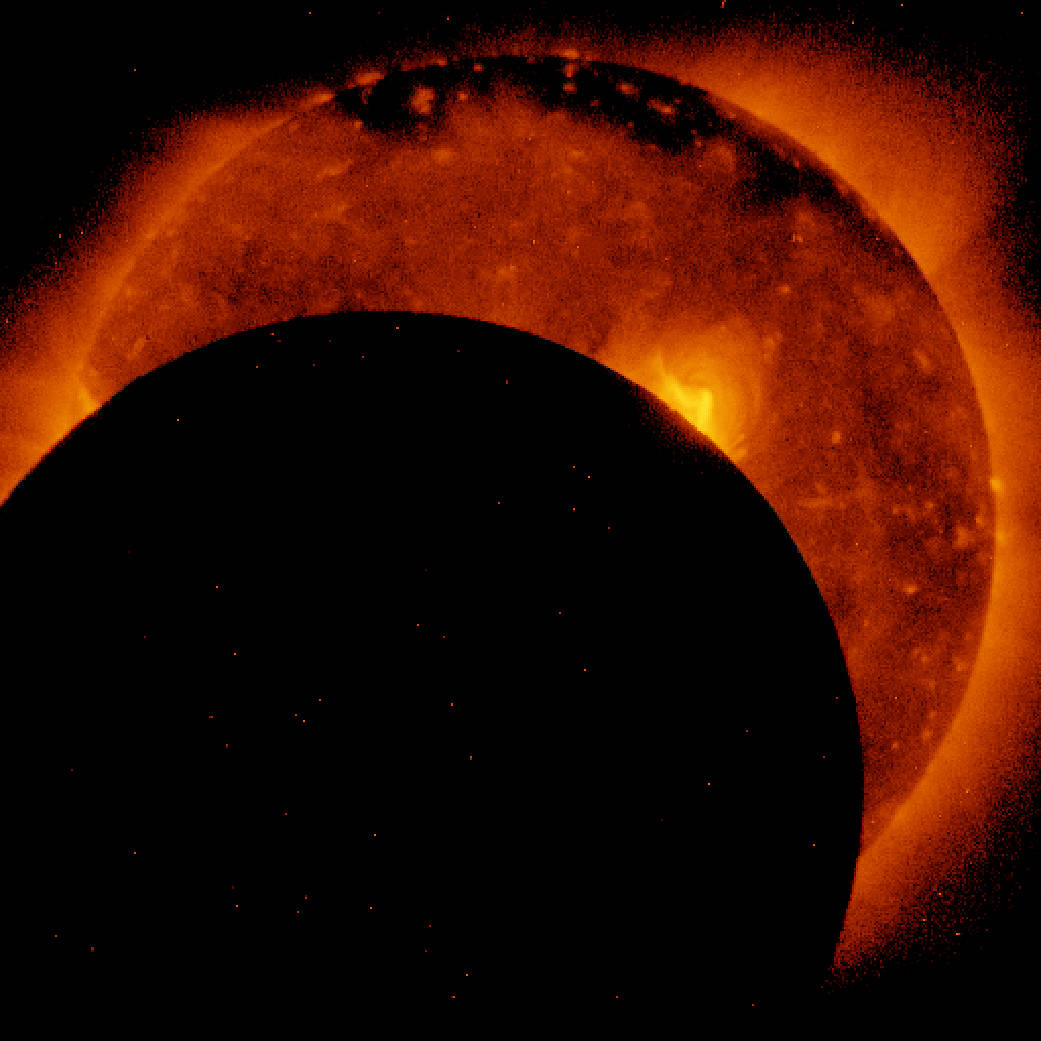
The eclipse last month brought a moment of cosmic uncertainty to the uninformed, although astronomers profess that the occurrence was totally predictable and certain, occurring completely over the continental United States. [Above picture from Hinode Solar Observatory Satellite JAXA/NASA. August 21, 2017.] My colleague Philip Ransley, who has split his career between pediatric urology and chasing the moon’s shadow, gave a lovely talk on lunar eclipses when he received the Pediatric Urology Medal from the American Academy of Pediatrics in 2002:
“There is a beautiful rhythm in moonrise and rhythm in sunset. But there is nothing to compare with standing high on the Bolivian Altiplano in the center of the cone of the moon’s shadow with sunset all around and the eclipsed sun hanging in the darkness. Here, the majestic progression of time is played out before your eyes. An eclipse is quite an extraordinary coincidence. The sun is 400 times larger than the moon. By coincidence it is exactly 400 times farther away, and so the moon just covers the sun. But beware! We live in special times. The moon is moving away from us by a few centimeters each year. That is more than a meter further away than it was when I started coming to AAP meetings, and after only 2,000 million more annual meetings the moon will have moved so far away it can no longer cover the sun.” [Ransley. Chasing the moon’s shadow. J. Urol 168:1671, 2002]
This geometric coincidence is a cosmic rarity of time and space. Science writer George Musser wrote: “In all the hundreds of billions of our Milky Way galaxy, few, if any, are likely to produce total eclipses like ours.” [NYT Aug 6, 2017. The great American eclipse of 2017.] Rare moments of eclipses once terrified our ancestors, jeopardizing their routine predictability of day and night. Mark Twain’s 1889 book, A Connecticut Yankee in King Arthur’s Court, tells of an engineer who, after a head injury, finds himself in 6th century England and convinces people he is a magician by using the tricks of modern knowledge, such as predicting the eclipse of 528. Edmund Halley in 1691 applied the name Saros, from an 11th century Byzantine lexicon, to the eclipse cycle of 6585.3211 days that predicts when nearly identical eclipses occur. Halley’s appropriation of the name may be technically inaccurate with respect to the number, but it has endured. The celestial dance of Sun and Moon, from our point of view as Earthly audience, produces spectacular moments of eclipse when the two bodies seem to become one. Knowledge transforms those coincidences from terrifying episodes of uncertainty to predictable occasions of beauty. [Above: lunar eclipse diagram, Tom Ruen. Wikimedia, public domain.]
Nine.

A transatlantic collaboration between Ann Arbor and Copenhagen, initiated 23 years ago by Dana Ohl and Jens Sønksen (above) culminated 2 years ago in Denmark with a conference branded as CopMich, and reconvened here in Michigan for 3 days last month with 50 excellent talks from junior and senior faculty of both institutions, plus our residents and fellows (below). Dana and Jens plan to continue this on a 2-year cycle, offset with our biennial Dow Health Services Research meeting. Our Andrology Division under Dana Ohl has grown to 4 clinicians including Jim Dupree, Miriam Hadj-Moussa, and Susanne Quallich Ph.D. (nursing). Jens spent a year working with Dana in 1994 and has maintained close ties with Michigan Urology. Our new residents room is named for Jens.

CopMich has expanded beyond andrology to include stone disease, voiding dysfunction, pelvic pain, and robotic oncology surgery with speakers from our department and the Department of Urology at Herlev and Gentofte Hospital and the University of Copenhagen, where Jens is Professor and Chair. Guest speakers were Manoj Monga, Director of the Stevan Streem Center for Endourology and Stone Disease at the Cleveland Clinic as well as the American Urological Association Secretary, and Chris Chapple of the Royal Hallamshire Hospital in Sheffield UK and Secretary General of the European Association of Urology. [Below: Manoj and Chris]

Michigan’s own celebrities spoke at CopMich program as well. Ed McGuire, emeritus professor and chief of urology (1983-92) and John DeLancey Professor of OBGYN have virtually defined the intellectual and clinical terrain of female pelvic medicine and pelvic floor neuroanatomy. Dee Fenner, like John, is also a joint faculty member of Urology and esteemed throughout the world. [Below: McGuire, Fenner, DeLancey]

The meeting, offering 15.75 CME credits, was underwritten by both academic units as well as ReproUnion and the Coloplast Corporation. Stig Jørgensen (below) represented ReproUnion and gave an excellent presentation on its funding mechanisms in Europe.

The Danish contingent was superb (partial contingent below) and, after all, there is nothing like a Dane (apologies to Rogers, Hammerstein, and South Pacific).

Ten.
My daughter Emily is an Irish literature scholar, so any mention of WB Yeats is likely to catch my attention, especially in an administrative meeting. This happened recently when Marschall Runge brought Dr. Fionnuala Walsh, former senior vice president of global quality at Lilly, to his regular meeting with the department chairs to describe the company’s quality journey to operational excellence. Her presentation perked me up with a reference to Yeats, specifically the last 2 lines in his 1928 poem Among School Children:
“O body swayed to music, O brightening glance,
How can we know the dancer from the dance?”
Novices like me can hardly guess exactly what Yeats had in mind with this thought, beyond the obvious conflation of performer and performance, but that’s the beauty of art in that one’s personal experience as the viewer or reader is where meaning is ultimately ascertained. Yeats also reflected on dance in other works, notably Sweet Dancer, a poem begging the audience to let the dancer “finish her dance.” [EC Bloom. W.B. Yeats’s Radiogenic Poetry in The Wireless Past. Oxford University Press. 2016] Sweet Dancer was first published as a radio play in 1937, a time described as Yeats’ “second puberty.” Yeats’s life, like most, intersected with urology and for him the coincidence most famously was his Steinach operation in 1934. [MA Kozminski, DAB. J Urol. 187:1130, 2012]
That metaphor of unity between art and artist surfaced again recently in a JAMA article by Kimberly Myers called The Paradox of Mindfulness: Seamus Heaney’s “St Kevin and the Blackbird.” [JAMA. A Piece of My Mind. 318:427, 2017] Myers reflected on the challenging impact of fatigue on a person’s attentiveness to responsibility and compassion and links the allegory of the medieval monk to the modern health care provider.
“One might say of the physician what St Anthony says of the monk: ‘The prayer of the monk is not perfect until he no longer recognizes himself or the fact that he is praying.’ … commitment to patient-centered medicine is noble, and it is arduous. And, as is true with any other clinical skill, perhaps it is only with years of practice and continual commitment to being one’s most authentic self in the work he is called to do that it becomes second nature, part of his very body, blood, and bones. Perhaps we are indeed most mindful when we are least aware of being mindful – to borrow a beautiful phrase from another Irish Nobel laureate, W.B. Yeats, when we no longer ‘know the dancer from the dance.’”
This idea brings me back to last month’s reflection on performance and the aspiration of going beyond mere competence to achieve excellence in one’s work. As medical faculty perform the work and study of health care while educating their successors, the moments of our performances are quantum bits of education for those who learn from us. Our best clinical and academic performances can inspire a future physician for a lifetime.
When we fall short we hope our observers have compassion for our human frailty, but that they are challenged to surpass us in their work. The extraordinary emergence, when a dancer achieves unity with a dance, is the very art of medicine that glues us together and inspires those who follow, now in the third century of the University of Michigan.
David A. Bloom
University of Michigan, Department of Urology, Ann Arbor

I continue to look forward to the arrival of my Matula Thoughts post each month. Greatly improves my knowledge and understanding of the world, along with my conversational mojo. Thanks!!!!