The University of Michigan Department of Urology
3875 Taubman Center, 1500 E. Medical Center Drive, SPC 5330, Ann Arbor, Michigan 48109-5330
Academic Office: (734) 232-4943 FAX: (734) 936-8037 www.urology.med.umich.edu https://matulathoughts.org/
|
What’s New November 1, 2013
Nesbit Society and Other Thoughts
A monthly communication to the faculty, residents, staff, and friends of the University of Michigan Urology Family.
31 Items, 1 Web Link, 15 Minutes
|
1. The autumn leaves are mostly gone, our PGY1s are well into their game, and our chief residents and finishing fellows are looking at their next stage of professional life. All these themes came together two weeks ago at our Nesbit Society Reunion. Although Hugh Cabot actually established urology at Michigan (circa 1919/1920), his trainee Reed Miller Nesbit, was the first formal section head from 1930 to 1968. Jack Lapides followed from 1968 to 1983 during which time his former resident and later colleague, John Konnak (Nesbit 1969 Trainee), spearheaded the Nesbit Society that formed in 1972. When Lapides retired in 1983 Ed McGuire came from Yale to become section head and brought me here from Walter Reed in 1984. Michigan Urology became an official department of the medical school in 2001 under Jim Montie, our first chair.
2. The Nesbit Society has a reunion and scientific meeting on campus in the autumn, usually around a football game in which, this year, Michigan prevailed after a challenging contest with Indiana. Additionally we have a reception at the spring meeting of the AUA, on Sunday night May 18, 2014 next year in Orlando. Membership is now at 211 active members (including our 3 new faculty members), 34 senior members, and 32 associate members. We have gradually been broadening the membership of the Nesbit Society to include not only our residency/fellowship alumni and our faculty, but also our UM undergraduates and medical students who found their way (inspired by Michigan Urology, one way or another) into the field. The Nesbit Society is an important bridge from our past to the future. We need to support that bridge, so if you missed the meeting this year, try to put it on the calendar in 2014 (October 9-11 when we will be playing Penn State). If you don’t quite think you are “a member” but have even a slight interest in coming to a great CME event, a great tailgate/football game, and a dinner with wonderful friends and colleagues – drop me a note, put it on the calendar, and come as my guest.
3. Three outside speakers and one colleague from our School of Business distinguished the program this year. Ray Costabile, Senior Associate Dean, Vice Chair and Professor of Urology at the University of Virginia spoke about his career in the U.S. Army and challenging work running “An Academic Medical Center on the Battlefield” as well as “Controversies in Andrology.” Both talks were crowd-pleasers. (Years back both Ray and I were at Walter Reed together). Jovan Ivchev, a friend of Michigan Urology for many years, gave “An Overview of Military Medicine in Macedonia and its role in NATO peacekeeping operations.” Jovan is Head of the Military Medical Service of the Army of the Republic of Macedonia and he is an accomplished urologist and general surgeon.
4. Dana Ohl had inserted an andrology theme into the Nesbit meeting that included his own superb talk and a terrific presentation of Rob Jackson [Nesbit 2012 and former fellow of Dana’s]. Rob is now in practice in Boise, Idaho. During his years at Michigan, with Julie and their children, he tried to visit each of our public parks and probably hit that mark or came very close. Ray Reilly, Professor of Business Administration at our Ross School Business spoke on “Managing your portfolio in turbulent times.” His pyramid of prudence (as I would describe his approach) was well-received by the audience, with an interesting counterpoint from our own Dr. Cheng-Yang Chang.

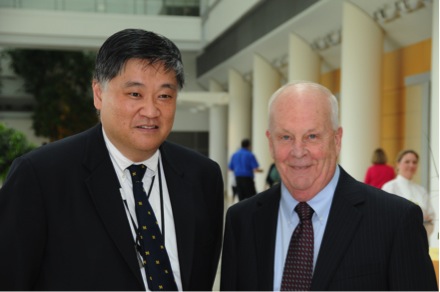
Joe Cerny [Nesbit 1962], Carl VanAppledorn [Nesbit 1972], Cheng-Yang Chang [Nesbit 1967]

Hugh Solomon [Nesbit 1980] and Meidee Goh [Nesbit 1998]

Julian Wan [Nesbit 1990] (President) and Ann Oldendorf [Nesbit 1992] (Secretary Treasurer)

Attendees at the Nesbit Society Meeting
5. At Nesbit we also heard a number of first-rate presentations from our residents, fellows and faculty. I gave the usual talk on the state of the department, that is solid after a rocky 2 years (much like the rest of the world) and explained why we need a substantial clinical margin (the faculty’s “tax” for running an academic program with education, research, and leadership centered around our essential deliverable of kind and excellent patient-centered care) in addition to help from our friends in the form of philanthropy. Medical research funding is shrinking. Ray Costabile was quick to note that the same pertains at his shop in Charlottesville: to get a dollar from the NIH has traditionally cost us a dollar-and-a- half. I expect very shortly (if not already now) we will revise that calculation and find it really takes more than two dollars to get one from the NIH. Research and discovery are essential to our field and our species, and we have been lucky to have had relatively easy money from the government in the past, those days are gone.
6. A similar story pertains for residency training (GME). Even with money we get from the Medicare-based funding of GME, we train more residents and fellows than the government pay supports. The bottom line is that our faculty practice and philanthropic base have been essential for the several million dollars we need each year to deploy the Michigan Urology mission of education, research, leadership, and that essential deliverable of kind and excellent patient-centered care. Michigan Urology has been doing this well for close to a century, even as rules, systems, and economics have changed. These things are changing again, faster and more substantially. Every iota of interest and support helps us, and every nickel contributed is stewarded wisely in support of our mission.
7. At the Nesbit dinner Friday evening Betty Konnak graced us with her presence. Dan Murtagh [Nesbit 1983] and his wife, Stephanie, (pictured below) joined us to celebrate his 30th class reunion.

Dan reminisced about his residency training days with John Konnak: to this day when he is doing a difficult case and has a moment of quandary he “hears” John’s admonitions “showing him the way.” Brent Hollenbeck [Nesbit 2003] celebrated 10 years. John Wei was awarded the 2013 John W. Konnak Faculty Service Award for his dedication to the educational, research, and service missions of the department. He was also honored this past week at the Faculty and Staff Awards Dinner on receiving the Dean’s award for Clinical and Health Services Research.
8. At the Nesbit dinner we also recognized Ed McGuire along with his wife, Susan, for service to the department. Ed was recruited to the University of Michigan as Professor of Surgery and Section Head of Urology in July of 1983 becoming Associate Chair of the Department of Surgery in 1988. In 1992 he joined the University of Texas Health Science Center at Houston as Professor of Surgery, and Director of the Division of Urology one year later. He returned to Michigan in July of 1999 as Professor of Urology and head of the Neurourology and Pelvic Reconstructive Surgery Division in the Department of Urology (a position he served as head until 2007). In 2007 he was named the Reed Nesbit Professor of Urology. In the past few years he shifted his effort to the Ann Arbor VA. On June 30 of this year Ed officially retired from the U of M and was granted Professor Emeritus of Urology status at the September Regents meeting. We honored Ed by giving him a collegiate chair (the kind you actually sit in). Ed will remain in our department as an active emeritus faculty and continue his work on the next volume of the history of urology, among other projects.
9. On a larger palette, healthcare USA remains a work in progress, but overall it is far below its potential. Yes, we have some, (arguably most), of the high points of innovation and performance in the world, but we fall short in terms of distribution, equality, and systemic integration. Many people experience terrible personal hardship when they fall through the cracks between silos of turfs and systems. Economic hardship is rife as people fall through the economic cracks of health care – I’ve heard the figure that more than 50% of personal bankruptcies are related to catastrophic health care bills. If you suffer a million dollar health care catastrophe, your 20% copay can make you homeless.
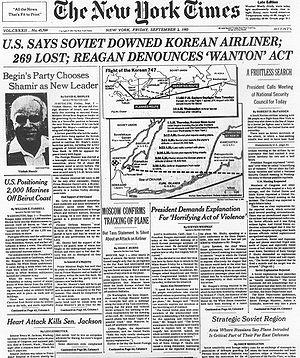
10. Bad press. A recent front page NY Times article profiled a 78 year-old lady in Florida needing a partial denture. The bill was $5700 and the dentist gave her a “special line-of-credit” with a financing company. It was good news for the dentist who was paid up front. The lady was given a payment plan at 23% interest that would go to 33% (plus a $50 penalty) if a payment is missed. Her minimum monthly payment of $214 takes a third of the Social Security check that she lives on. [Silver-Greenberg J. “Patients mired in costly credit from doctors.” NYT Oct 14, 2013. CLXIII p. 1] Of course dentists need to be paid fairly and of course many elderly people need dentures. But this common scenario doesn’t seem right – and notice that the caption of the article says “doctors.” The public is increasingly unhappy with all health care professionals.
11. The ACA – how is it working? The point to make is that the law is here, it’s not going away, and it is (in spite of its many problems) a natural progression of health care legislation on this country. The ACA has been in place and in play for over three years. It is certainly imperfect and contains mistakes, omissions, and glitches, but it is the third major installment of the federal determination of health care that started in 1935 with the Social Security Act, extended in 1965 with the Medicare/Medicaid Act, and expanded again nearly on a 30-year cycle in 2010. The law is an attempt to make health care accessible, affordable and accountable to patients. You can look at the law as a bridge between patients and health care, although perhaps it is more of a causeway constructed of various pathways of insurance carriers and federal programs. Whether you like it or not, it is here after due process, it fills many needs of the public, and it needs to be improved as it gets implemented. It made no sense to try to turn back the hands of time and hijack the national economy in the hope of reversing the law. The national model of health care that may have worked well enough at the end of the 20th century cannot be parbuckled.
12. Clearly the roll-out of the sign-up phase for the health care exchanges was marred by immature, clunky, and poorly fashioned software products, but we understand that already well-enough in the daily work of health care especially here in Ann Arbor. Actually, if I have any overarching complaint it is with the HITECH law and ICD 10 that preceded the ACA, and mandated systems that have slowed down health care delivery, driven up costs, enriched a few companies beyond imagination, and turned provider-patient relationships into forced encounters tailored to satisfy federally-determined “meaningful uses.” A cover illustration from JAMA last autumn, drawn by a little girl observing her sister’s visit in a doctor’s office, tells the story better than ten thousand words. Notice the doctor’s position and attention. [JAMA, 307(23):2497, 2013]

13. “What’s New”, that you are reading now, began over a decade ago in the Dean’s Office here at Michigan under Allen Lichter when faculty, and most other people on the planet, were becoming deluged by information. Heavy activation of the “delete” button was the only way to get home at night, and even then to get to sleep. The right index finger of Homo sapiens was developing more callus and bone density around the world wherever anyone had access to a computer. It seemed to us then that a single predictable message that filtered and digested a minute fraction of useful information from the 2.5 exabytes (2.5 x 1018) of data produced by mankind every day would be welcomed. In the Department of Urology, we have an internally-directed “What’s New” every week, targeted mainly to faculty and residents, but often filled with internal operational issues and intended as weekend “homework.” In these over the course of each year we hear from our divisions and our individual faculty members who produce their own editions of “What’s New.”
14. On the first Friday of each month (such as now) “What’s New” has a broader message and distribution, going out to the entire department, alumni, friends, colleagues, and other curious souls who sometimes send me very welcomed thoughts of their own. One of the objectives of What’s New is to be an electronic mini-journal club. We each read a unique set of newspapers, magazines, journals, and books so I hope whoever produces one of these weekly issues will digest one or more articles, ideas, or factoids from the daily 2.5 exabytes at large and share them with the rest of us. As the email chain for “What’s New” got longer and longer we started also posting this as a “blog” at MatulaThoughts.org. We are still in the learning stage of the blog-o-sphere, and are finding our way in it, but we hope you come to find MatulaThoughts.org easier to access and read.
15. Factoid of the day number one. On this day in 1957 the Mackinac Bridge opened to connect the two pleasant peninsulas of Michigan. This was then the world’s longest suspension bridge between anchorages. The main span is 3,800 feet, making it now the third longest suspension span in the U.S. and the 15th worldwide. However, the entire 8,614 foot bridge is the world’s third longest in total suspension and the longest between anchorages in the Western hemisphere. The maximum height above water is 552 feet. The Verrazano-Narrows Bridge, opened in 1964, has a span between towers of 4,260 feet, a maximum height of 228 feet. The Golden Gate, opened in 1937, has a center span of 4,200 feet, a span between anchorages of 6,463 feet, and a maximum height of 746 feet. Longer anchorage-to-anchorage spans have been built in the Eastern Hemisphere, including the Akashi Kaikyō Bridge in Japan (12,826 feet). But the long lead-ups to the anchorages on the Mackinac make its total shoreline-to-shoreline length of 5 miles longer than the Akashi Kaikyō (2.4 mi or 12,672 feet). Like most things, it all comes down to definitions and clarity when you talk about bridge lengths. The main span between towers, the distance between anchorages, and the shoreline to shoreline lengths are all quite distinct.
16. The big three American suspension bridges. (The U.P. is still a bargain.)
a. Mackinac Bridge $4.00 each way, daily traffic 11,600.

b. Verrazano-Narrows. $15 each way, daily traffic 189,962.

c. Golden Gate. $5 northbound only (southbound no charge), daily traffic 110,000.

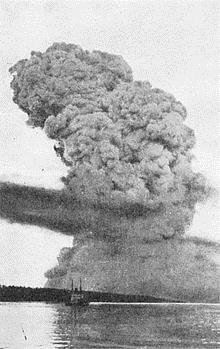
17. Interesting things happen under bridges and on the sea, and in that respect parbuckling is a word that entered my vocabulary recently. It refers to the righting of a disabled ship, the notable case being the Costa Concordia on September 17, an amazing feat of determination, strategy, technology, and teamwork. The hapless individual responsible for the disaster itself, namely the captain of the ship, recently went on trial in Italy. Is he just a scapegoat for larger business decisions of the corporate enterprise that employed him or was the responsibility for the specific misadventure his alone? Like most binary questions of business, the answer is split between the choices. His selection and the culture of the organization may have set the stage for the SNAFU (I love that old Army acronym), but unquestionably it was the captain at the end of the sad day who steered that ship into the ground.
18. Parbuckling may expand in its meaning to encompass the concept of resurrecting an entity or enterprise that while perhaps iconic in its day may be flawed enough to prohibit survival in new Darwinian circumstances. The Titanic is another relevant maritime metaphor. Like the Costa Concordia it was an amazing piece of technology for its time with hundreds of thousands of parts and thousands of processes. However, an overconfident captain, faulty systems of command and control, and structural deficiencies led to disaster. Who actually was responsible in each case? We have yet to build a perfect system on which we can rely that does not require the human factor. Maybe you might think Voyager 1 and 2 might qualify as examples, but even they will run out of power one day, and likely needed some tweaking along their incredible journeys up to now. Parbuckling won’t save them when that power runs out, nor could it save the Titanic. Anyway, leadership matters.
19. Factoid number two (you can use this one): cranberries and UTIs. A JAMA Clinical Evidence Synopsis by Jepson et al concluded that cranberry products are not associated with UTI prevention. This seems to explode an old belief of mine, although the authors qualify their claim that a lack of sufficient active ingredient or statistical powering may have influenced their analysis. [JAMA 310:1395, 2013]
20. Another useful factoid: anti-oxidant supplements are not associated with decreased mortality and beta carotene, vitamin E, and higher doses of vitamin A may be associated with increased mortality. This comes from another JAMA Clinical Evidence Synopsis. Bjelakovic et al came up with this conclusion after an analysis of 78 RCTs involving nearly 300,000 participants. [JAMA 310: 1178, 2013]
21. Continuing the idea of the electronic journal club, I can’t mention JAMA without bringing up the October 16 issue that has two contributions from Michigan. First is a paper by Steven Katz, and Sarah Hawley from our Departments of Internal Medicine and Health Management and Policy. This Viewpoint piece is entitled: “The value of sharing treatment decisions making with patients. Expecting too much?” [JAMA 310:1559, 2013] The authors dissect the idea of “shared decision making” (SDM). Like many simplistic solutions to complex problems, the unintended consequences may exacerbate the original problems. The authors conclude: “…too little is known about SDM and its outcomes to support its role in addressing the increasing concern about overtreatment and medical cost inflation.” In other words, let’s not be too quick in inserting the “health policy idea de jour” into legislation and funding methodologies. The experience and damage from HITECH should offer enough evidence to avoid helter-skelter and knee-jerk health policy formulation. You can hear Steven’s on-line interview at Online@jama.com.
22. Also in that edition is an editorial by Preeti Malani from our Department of Internal Medicine “Preventing infections in the ICU. One size does not fit all.” [JAMA 310:1567, 2013] This editorial responds to a paper in that same issue on a randomized trial in 20 hospital ICUs to see if gloves and gowns mattered at all in acquisition of MSRA or VRE. In this study of 26,180 patients health care workers in one cohort used gowns and gloves for ALL patient contact, whereas the workers in the other cohort used only “usual care” unless an individual patient had known infection with antibiotic resistant bacteria – in which case gowns and gloves were worn in compliance with CDC guidelines. The study, by Harris from the University of Maryland School of Medicine, showed no difference in outcome regarding MSRA or VRE acquisition. Preeti’s editorial advocates caution in interpreting the finding and tailoring any approach to “the epidemiology of specific ICUs and resources available.”
23. The Lancet is another journal I try to skim with regularity (I depend on others to read the high-fluting New England Journal of Medicine) and as I was thumbing through the Sept 28-Oct 4 edition I found a strong imprint of the University of Michigan. John Birkmeyer and his group have two articles on “Variation in Surgery.” He is lead author of the first that studies regional variation in surgery [Lancet 382:1121] and senior author on Peter McCulloch’s paper on strategies to reduce variation in the use of surgery [Lancet 382:1130]. The first article is the source of the “cover quotation” that distinguishes most issues of Lancet: “A patient’s odds of undergoing surgery often depend more on where he or she lives than on clinical circumstances.” In the same issue of Lancet Regina Morantz-Sanchez, of our history department, has an article in “The Art of Medicine Section” on Mary Amanda Jones one of the rare early women gynecologists in the male-dominated world of surgery in the later 19th century [Lancet 382:1088, 2013].
24. Scientific literacy 101: Nobel Prize in Physiology or Medicine 2013. This went jointly to James Rothman (now at Yale – work done at Stanford, MMSK, and Columbia), Randy Schekman (a Howard Hughes Investigator, now at UC Berkeley – work done at Stanford and UC) and Thomas Südhof (also a Howard Hughes Investigator now at Stanford – work done at UT Southwestern) for discoveries related to vesicle traffic mechanisms in cells. The intracellular control of “cargo” is a matter of exquisite logistics, the term that United Parcel Services (UPS) has leveraged so nicely in its advertisements. While UPS and its sister organizations manage your Amazon purchases, our intracellular vesicles manage hormones, neurotransmitters, enzymes, cytokines, etc. getting each one to the right place, at the right time. Schekman identified three classes of genes that regulate this work. Rothman discovered the membrane docking and fusing mechanism that works via protein complexes. Südhof identified how “temporal precision” is achieved by calcium sensitive proteins that activate a zipper like mechanism at the outer membrane of a nerve cell. This is important in all parts of biology, but especially so in our area of neuro-urology.
25. One of the things that bothered me about the significant recent legislation related to health care, including such things as HIPPA, HITECH, and ACA is that the voice of our profession was drowned out by input from large corporate interests of third party payers, hospitals, big pharma, and other large industries of health care. The big special interests, seem to have eclipsed out the interests of the “house of medicine.” Part of the responsibility for this situation lies with us insofar as I think most of us medical professionals have a skewed perspective on the business of lobbying – a distaste for it – and accordingly our profession has a very weak voice in Washington. We should get over the distaste.
26. The Constitution protects even our weaker voices, relative to big corporate interests. This protection comes in the Bill of Rights with the First Amendment that secures five freedoms: those of speech, the press, religion, petition, and assembly. The right to petition of government is essential to a democracy. Citizens have general interests and special interests. Those general interests such as life, liberty, and the pursuit of happiness apply to all citizens, but special interests need protection as well because, after all, we are all specialists of one sort or another whether plumbers, panhandlers, pianists, or pediatric urologists.
27. Urologists have two important professional organizations. The most immediate is the AUA (American Urological Association) that was established in 1902. The ACS (American College of Surgeons) dates back to 1913. These organizations were formed to consolidate the professionalism and values of their members and to further their education in the changing world of science, technology, and healthcare. The public interest of these goals and functions is represented in their tax-exempt nature as 501c(3) organizations. However, such identification prohibits their ability to engage in the political activities of lobbying for their special interests by means of supporting political candidates. Accordingly, the ACS in 2001 and the AUA in 2002 set up political action organizations under the 501c(6) tax code. These PACs were established as bridges between the members of their professions and federal officials. By law individuals such as us can contribute up to $2,000 per year while the PAC can contribute $5,000 per candidate per election cycle. Only the members of the AUA and ACS can contribute to these two PACS. The AUA-linked organization has recently reached the million dollar level of total annual funding while the ACS group is at about the $600,000 level. Although the scale of these PACs may seem small, they have a relatively larger impact in the halls of Congress because of the very nature of their representation of finite groups of professionals. Representatives are receptive to these authoritative professional groups. Interestingly – the UM Health System PAC representing our enterprise at home has less than a “$12,000 yearly voice.” You’d think it could be stronger.
28. To me, the ACS political committee represents our general interests as surgeons, while the AUA political arm represents our special interests as urologists. Both sets of interests are compelling and certainly overlap. While the ACS may, for example, lobby for standards of trauma units, GME funding, etc. the AUA political group might focus on such specific things as constraints on PSA usage, lithotripter deployment, and guidelines implementation. All these things and many more represent legitimate objectives of not only the professional aspects of urology, but just as well and even more importantly of the needs of patients with genitourinary conditions. The aligned interests of these two conjoined groups, urologists and patients, are nowhere represented better anywhere else. Still, the involvement of surgeons and urologists in these two agencies is sparse – only 3.5% of ACS members and somewhat better for the AUA membership in its organization UROPAC. In contrast to the Mackinac Bridge the tariff on our bridges to federal legislation is up to an individual’s discretion up to the legal limit of $2,000 per year.
29. Healthcare exchanges, ACOs, and direct business-health systems bridges. These new things are replacing the traditional individual insurance-based/employer-supported form of health care. One form or another of these experiments in health care delivery was bound to happen with or without the Affordable Care Act. Some prominent direct business-health systems bridges include Walmart and GE. Walmart and Lowe’s joined the Pacific Business Group on Health Negotiating Alliance to create the Employers Centers for Excellence Network that will offer no-cost hip and knee replacement for more than 1.5 million employees and dependents at Johns Hopkins Bayview, Kaiser at Orange County, Mercy Hospital in Springfield, MO and Virginia Mason Clinic. Other similar bundled payment direct contract may occur with Cleveland Clinic, the Mayo Clinic and Geisinger Clinic to provide care for employees with specific higher end specialty needs.
30. Close to halfway up towards the Mackinac Bridge you might stop in the territory of MidMichigan Health, a quality healthcare system with a number of links to Ann Arbor. Those links have been strengthened by a significant affiliation that is being developed through an organizing council with 8 members of each institution. Furthermore, 2 members from UM have joined the MidMichigan Board, these being David Spahlinger, our Senior Associate Dean and leader of the Faculty Group Practice, and Doug Strong, our Chief Executive Officer. An oncology council, a heart and vascular council, plus additional collaborations in Ob/Gyn, Neurosurgery, Pathology, Radiology, Telemedicine, IT, Palliative Care, and Case management are already in play. Credentialing/privileging standards plus quality/safety systems are also being brought together. We expect this relationship to improve both health systems.
31. Last month our internal weekly “What’s New” profiled Mike Kozminski in the General Urology Division; Florian Schroeck and Paul Womble, fellows in the Urologic Oncology Division, and an update from John Wei our Director of Communications, Marketing, and Networking. Website: http://www.med.umich.edu/urology/about/MonthlyNewsletter.html. Also at the recent AUA North Central Meeting we had several people win awards. Florian Schroeck had two awards: (1) Traveling Fellowship Award of the North Central Section of the AUA for the manuscript entitled “Regional Variation in Prostate Cancer Quality of Care” and (2) Best poster in the Outcomes / Socioeconomics poster session for the abstract entitled “Technology Diffusion and Diagnostic Testing For Prostate Cancer.” Miriam Hadj-Moussa, HO3, won 1st place in the Bladder Malignant/Stone Disease/Endourology Poster Session for the abstract “Outcomes following radical cystectomy for bladder cancer in patients under 60 years old.” John Stoffel was selected as one of the scholars for the 2014 AUA/EAU Academic Exchange Program.
Best wishes, thanks for spending time on “What’s New” this first weekend of November. Your comments are welcomed.
David A. Bloom, M.D.
The Jack Lapides Professor and Chair
Department of Urology
TEL: 734-232-4943
Email: dabloom@umich.edu

 For centuries we have known that many diseases are contagious. Flags were routinely flown from ships to warn a town that disease was on board. The idea of quarantine comes from 17th century Venetian term quaranta, indicating the 40-day waiting period on ship to be certain that no active communicable disease was present before disembarking. Yellow flags have a long history of marking locations of disease, although green, black, or even a skull’s head have been used. The Lima (L) flag, or yellow jack is still in use, although yellow jack was also a name for yellow fever. A plain yellow flag (Quebec or Q) may have also been so used in the past, but as meanings change with the times, today a plain yellow Q flag means a ship is free of disease and can be routinely boarded and freely disembarked. We are somewhat insulated from the stark terror that infectious diseases inflicted on populations, not so long ago. A gathering storm of Ebola virus or renewed treachery from influenza may resurrect the ancient panics of lethal infectious diseases. Our colleague Howard Markel in the department of Pediatrics, wrote an excellent book called Quarantine! in 1997, that is well worth a place on your shelf.
For centuries we have known that many diseases are contagious. Flags were routinely flown from ships to warn a town that disease was on board. The idea of quarantine comes from 17th century Venetian term quaranta, indicating the 40-day waiting period on ship to be certain that no active communicable disease was present before disembarking. Yellow flags have a long history of marking locations of disease, although green, black, or even a skull’s head have been used. The Lima (L) flag, or yellow jack is still in use, although yellow jack was also a name for yellow fever. A plain yellow flag (Quebec or Q) may have also been so used in the past, but as meanings change with the times, today a plain yellow Q flag means a ship is free of disease and can be routinely boarded and freely disembarked. We are somewhat insulated from the stark terror that infectious diseases inflicted on populations, not so long ago. A gathering storm of Ebola virus or renewed treachery from influenza may resurrect the ancient panics of lethal infectious diseases. Our colleague Howard Markel in the department of Pediatrics, wrote an excellent book called Quarantine! in 1997, that is well worth a place on your shelf.
 Speaking of flags, Congress on this date, 4 April 1818, adopted a national flag standard with 13 alternating red and white stripes (for each of the original colonies) and a star for each of the 20 states at the time. This was the suggestion of U.S. Naval Captain Reid with a new star to be added for each new state. Up to then then no official standard existed and the number of stripes had grown to 15 with no particular arrangement of the stars specified. A number of variants were then in use including the circular arrangement of stars of the so-called Betsy Ross flag. The blue square, by the way, is called “the canton” in flag-speak and even Reid’s model allowed variable arrangements in the canton.
Speaking of flags, Congress on this date, 4 April 1818, adopted a national flag standard with 13 alternating red and white stripes (for each of the original colonies) and a star for each of the 20 states at the time. This was the suggestion of U.S. Naval Captain Reid with a new star to be added for each new state. Up to then then no official standard existed and the number of stripes had grown to 15 with no particular arrangement of the stars specified. A number of variants were then in use including the circular arrangement of stars of the so-called Betsy Ross flag. The blue square, by the way, is called “the canton” in flag-speak and even Reid’s model allowed variable arrangements in the canton.