WN/WN/MT Aug 2020
Folly & Truths
2472 words

One.
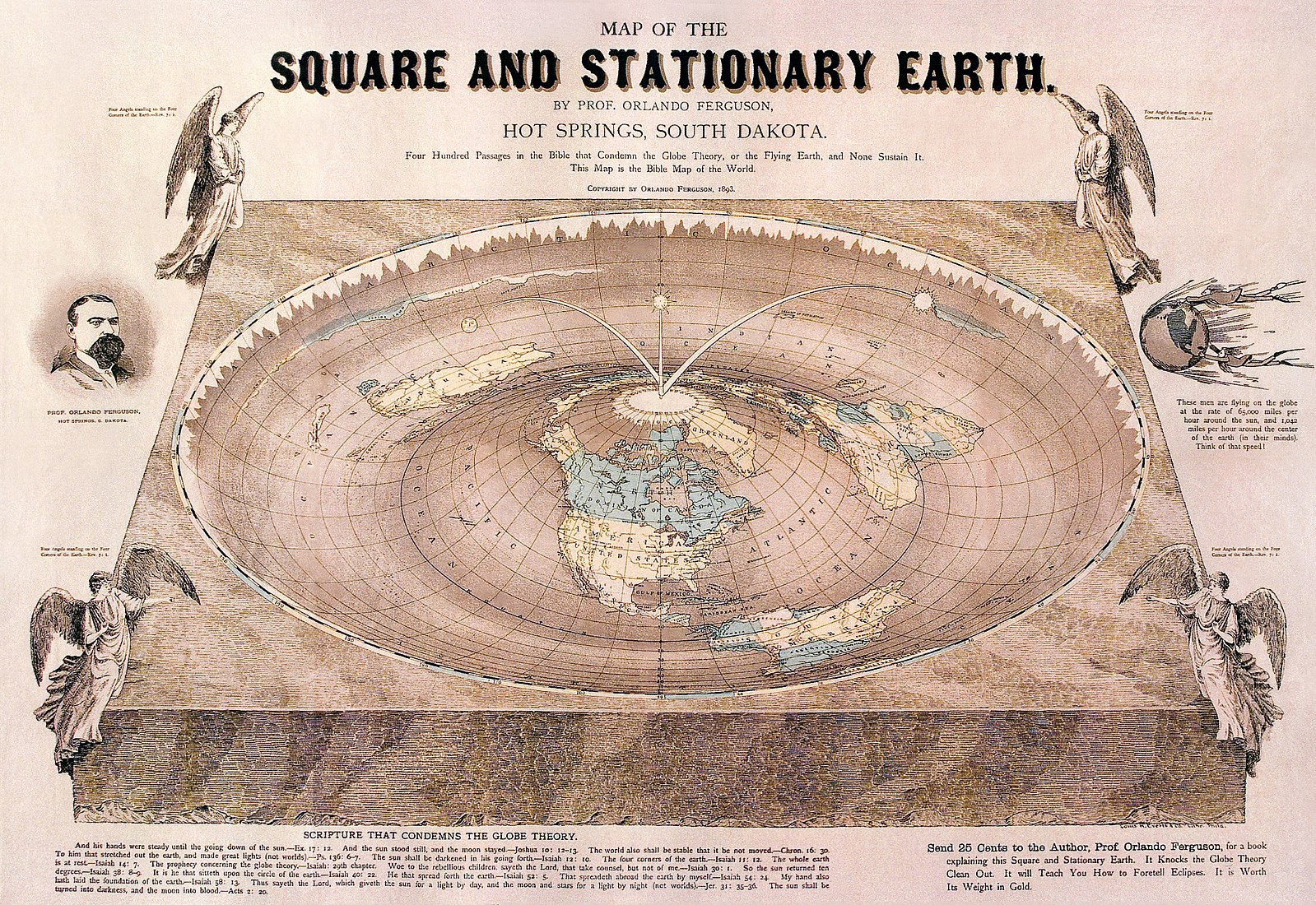
The Cure of Folly. Overwhelmed by insanity, the world might be a better place if we had a surgical cure for madness, but alas, surgeons can’t fix everything or everyone. Hieronymus Bosch (c. 1450 – 1516) imagined this scene around the time Christopher Columbus made his second voyage to Caribbean Islands and just before John Cabot was the first known European on the North American mainland – journeys that to “Flat Earther believers” seemed examples of pure folly. [Above: detail from The Cure of Folly, Museo del Prado, Madrid.]
Belief that removal of a “stone” in the head could cure “madness” was one of many unscientific ideas of humanity that spawned strong believers and industries. Such “stones” might have been actual subcutaneous nodules or more deeply-situated objects imagined in the brain. Factoids lurked behind fantasy, as so happens with many other follies. Bladder stones, for example, surely were real and caused grief. These unmitigated miseries could be relieved only by lithotomy, for patients lucky enough to survive the horrible experience of surgery without anesthesia, extensive blood loss, and likelihood of postoperative sepsis. No such evidence of relief exists for relief of mental illness by removal of scalp nodules or drilling into the skull by trepanation, beyond a placebo effect. Surgical cure for insanity, was an insanity itself, as Bosch’s painting attests, where he not only visually spoofed the bizarre idea of surgical cure of madness, but also implied a cure to the folly, in the operating theater of public opinion by means of the satirical title.
How does an individual gain confidence or belief in an idea, a skill, or a technology? The discernment of the utility of some thing or the truth of an idea is a critical function learned in childhood and honed throughout life. An open mind that is willing to learn and unconstrained by ideology helps this arbitration. A mind further trained by education and critical analysis improves the odds of giving fair measure to an idea, skill, or device. Humans have had countless ideas and inventions, but for any of these to persist in society they must be tested in commercial and intellectual marketplaces and reconciled to public belief and utility. An idea or technology sticks around when enough of the public – a quorum – becomes confident of its value and truth.
During a recent virtual pediatric urology meeting, in discussions over ideas of validity and truth, Julian Wan reminded us: “there are three types of arguments – the nature of relevant knowledge at hand; pragmatism; and sectarian belief.” As the tagline for The X-Files once promised: “The truth is out there,” although it’s not the same for everyone.
The large contest in play for H. sapiens today, is the ability of people to coalesce around some shared sense of basic truths that enable them to discern and choose between authoritarian societies versus representative democracies. This matter is especially intense now in this interconnected and fragile world where our technologies can distort truth and physically destroy the planet.
Two.
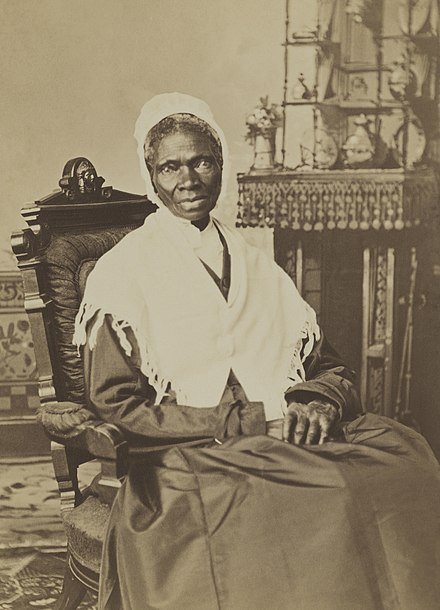
Truth. Isabella Baumfree is a timely person to consider. Born into slavery in a small Dutch-speaking community in the Catskills around 1787, she grew up known as “Belle.” Although New York state began to abolish slavery in 1799, emancipation was not complete until July 4, 1827. Belle “escaped” just before this, in 1826 with her infant daughter, but she preferred to say that she “walked off,” anticipating the emancipation. She had to leave three other children behind and two years later she went to court to recover her son, then five years-old and enslaved in Alabama. Remarkably, she won. In 1843 she renamed herself Sojourner Truth and became an abolitionist and women’s right’s activist. Her speech in 1851 at the Ohio Women’s Rights Convention in Akron “Ain’t I a woman?” established her celebrity and was reiterated widely throughout the years of the Civil War. Sojourner Truth moved to Battle Creek, Michigan, in 1857 and died at home in 1883. [Picture above, National Portrait Gallery, c. 1870.]
Sojourn, of course, describes a temporary stay or condition and the extraordinary name Sojourner Truth, writ large, implies a traveler who experiences various postulations of truth in pursuit an ultimate best version of it, through their days and times. The conditionality of facts and truths is not just a matter for philosophers – it is the daily work of historians and scientists who seek to disprove established beliefs (and follies) with better facts and reasoning. Sojourner Truth’s name is a fitting metaphor for the conditionality of truth, whether ascertained by ideology and sectarian fiat or by observation and reasoning, and even once ascertained it is always amenable to further examination.
Three.

History and science are good antidotes to folly, provided that their logic trumps the ideologies and beliefs that so often constrain people. Folly is the antithesis of good history and science. It is, by definition, foolish – lacking defining characteristics of our species: good sense, reason, prudence, and foresight. The rigor of history and science brings verifiable data and rational argument to old beliefs, in pursuit of the idea of truth. This pursuit depends upon free inquiry, free speech, peer review, criticism, and public education – all characteristics of open societies and the institutions sustain those societies. Ultimately, however, the cure of folly requires that people change their minds, based on data, analysis, and argument.
Governments, universities, industries, and all businesses, as they serve themselves, also serve the public interest and their integrity is tied to the public trust. Naturally, our expectation is that self-interest for industry and business is usually greater than their public service, but for governments and universities the public interest should dominate. Good science and good history (in the sense that “good” captures the idea of truth and reflects fundamental values of humanity) do not necessarily find nourishing soil in authoritarian societies, universities, corporations, or “top-down” organizations. In fact, authoritarian government has never worked well for people, history, or science. [Above: The Alchemist, Mattheus van Helmont.]
Society’s instruments, namely its governments, universities, and businesses, too often maintain stubborn illiteracy of history and science. These organizations ignore some truths that are becoming very clear with massively-accruing evidence of basic facts: infectious diseases recur in catastrophic waves, people need basic securities, and human environmental impact is deleterious to a human future. One wonders, then, what are the actual purposes, the main value, of those institutions (governments, universities, businesses, the press, etc.) to “we, the people?” Limiting the question just to government (recognizing that a huge body of scholarly work, beyond capacity of this writer and essay, continues to study this question). The Declaration of Independence, states it simply:
“… in order to form a more perfect union” so as to protect the basic human aspirations for “life, liberty, and the pursuit of happiness.”
Government facilitates these aspirations most fundamentally through basic securities of public safety, public education, assurance of jobs and justice, as well as public and personal health. Security of food and shelter are no less important, as this Covid epidemic is showing. These are the needs of “We, the people.”
Four.
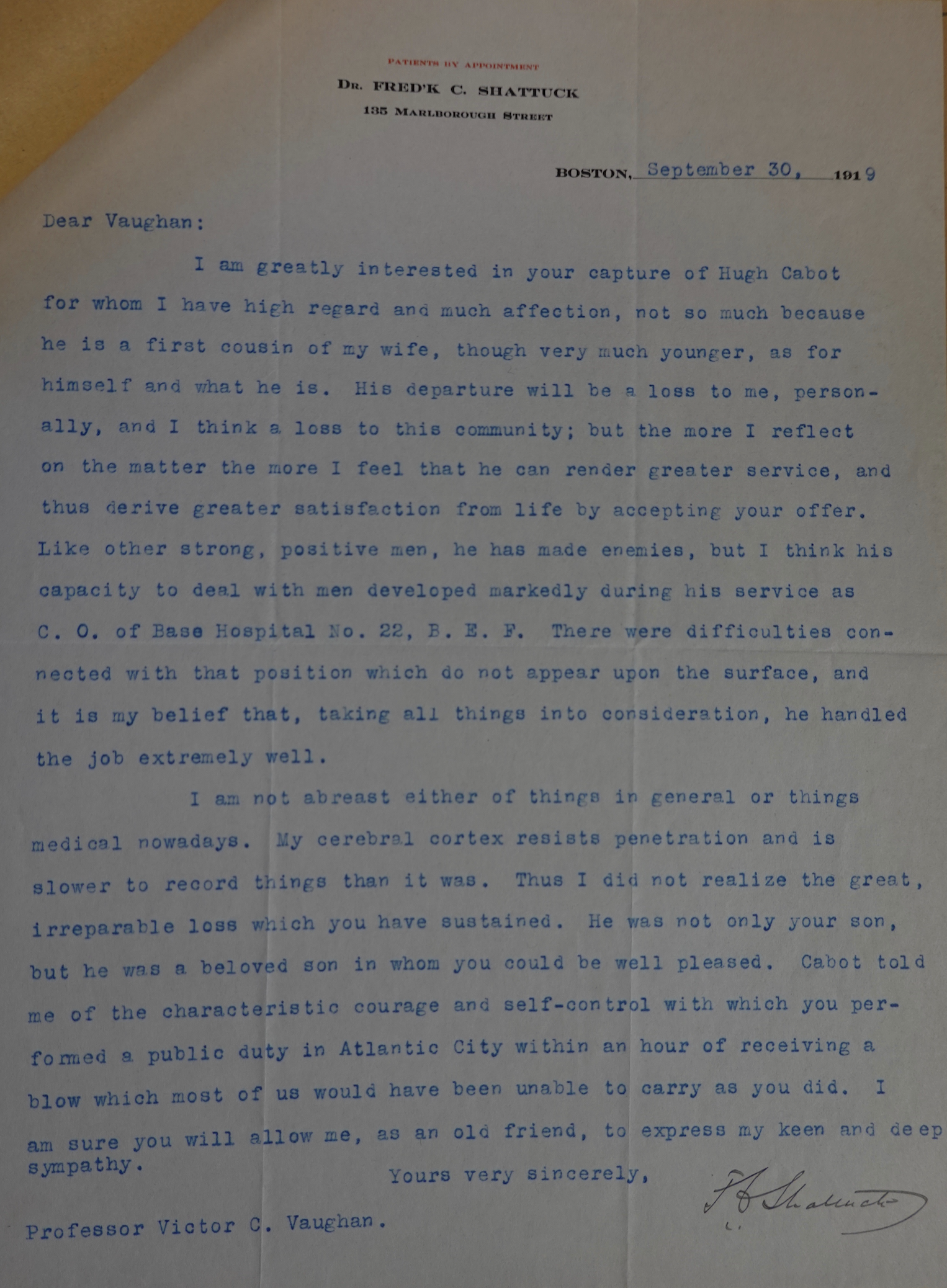
New medical students just joined us in Ann Arbor, although the absence of our usual White Coat Ceremony at Hill Auditorium deprived us of the chance to see them on stage, hear their introductions, and give them short white coats, stethoscopes, and MCAS pins. Cliff Craig recently sent Matula Thoughts a note recalling his precise moment of entry in 1969, before the White Coat Ceremony was introduced to our medical school. Cliff and his fellow students assembled to hear the dean, without any family members, children, or friends on hand to offer support and cheers, as would come with the White Coat event years later. [Below: Cliff c. 2019.]

“It was 1965, the first day for the University of Michigan Medical School class of 1969. We saw no white coats, nor short ones either. Dean Hubbard said (paraphrased): ‘You are all worried about failing out, I am not worried about that. I am worried that some of you will be bad doctors, and I wish I knew who you were, I’d kick you out right now.’ That was immediately followed by our first class; – so much for class ‘bonding.’
One year later, in 1966, on the first day of our second year, we were all advised to show up with a short white coat which could be purchased at Ulrich’s (along with the books we needed for the second year). It was a year punctuated by many demonstrations and sit-ins on campus against the Viet Nam war (Tom Hayden etc.). Dean Hubbard then addressed us again (paraphrased): ‘I want you to remember when you wear your white coat, you represent not only yourself but this medical school, the medical profession, but most importantly you represent me! If you want to participate in any of the activities on central campus, take off the white coat.’
I met Dean Hubbard at commencement in the early 2000s, and reiterated what he told us on those occasions. His response: ‘Did I really say that?'”
Time passed and now Cliff is professor at UMMS, specializing in the pediatric orthopedics. He keeps in touch regularly with several classmates including otolaryngologist Mike Johns, who served UM brilliantly as interim EVPMA after being Dean of the Medical School at Johns Hopkins and then Chancellor of Emory University. Rick Rapport, another classmate, is a retired neurosurgeon in Seattle.
Five.
William Hubbard was the first “full time” dean at UMMS, in the sense of having no conflicting duties such as departmental chair (like Cabot) or clinical practice (like Furstenberg). Hubbard served from 1959 through 1970, resigning to become a senior vice president at the Upjohn Pharmaceutical Company in Kalamazoo. Just the year before, the regents had given him responsibility as dean to also manage the hospitals of the growing medical center.
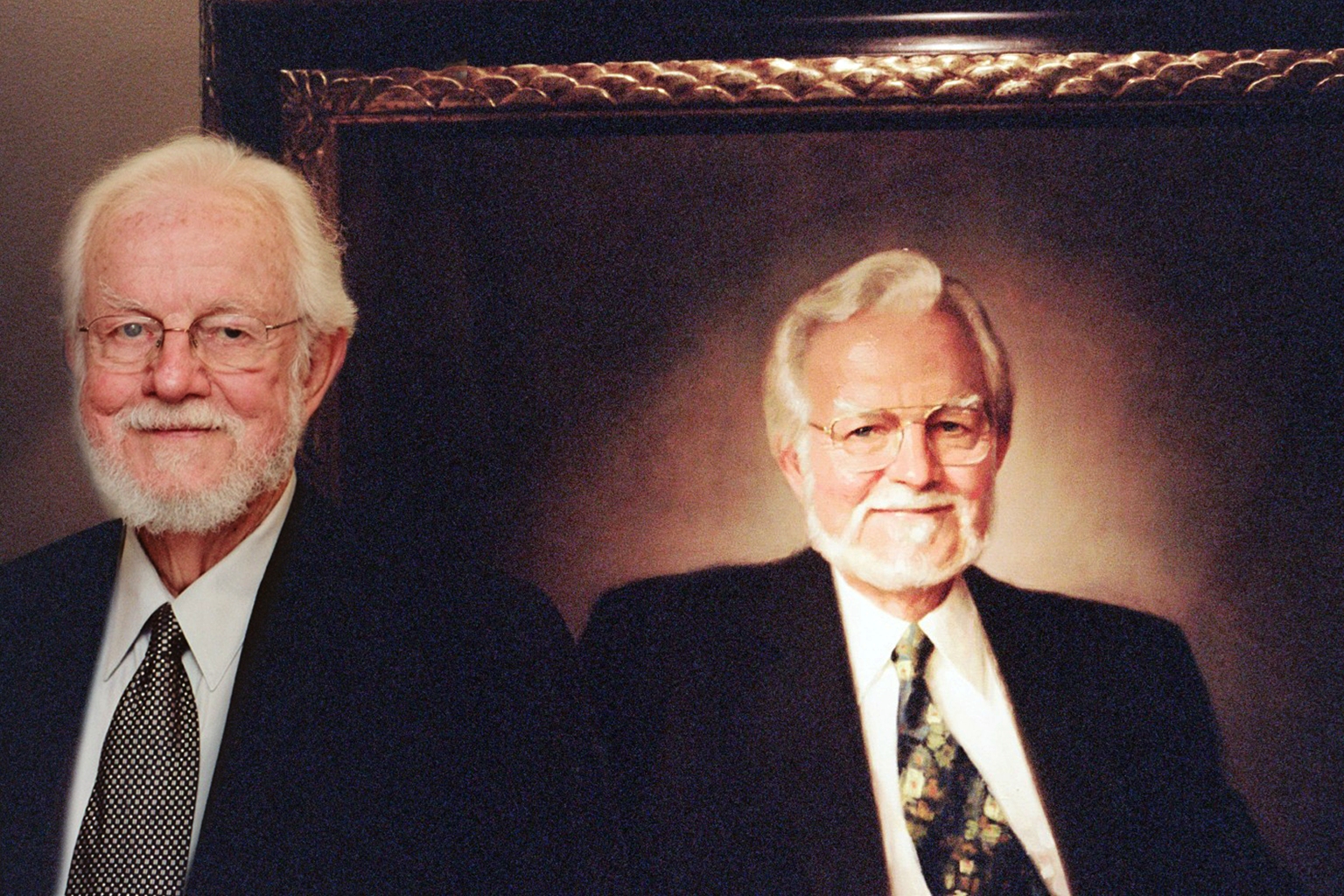
One evening in March, 2006, after usual work hours, voices were heard in the otherwise quiet hall outside the office of the Associate Dean for Faculty Affairs, who was curious to see who was wandering about in the administrative area of Dean Allen Lichter. This led to the good fortune of meeting former Dean William Hubbard who had come by to view his portrait. Fortunately, a camera was nearby to capture Dr. Hubbard and his painting from more than 30 years earlier. Fashions change and our deans’ portraits are now in storage. It was fortunate to have been hanging when history was still on display when Dr. Hubbard strolled by and he seemed pleased to reflect back on his time at Michigan. It is too late to ask Hubbard to recall his memories of Nesbit and Lapides, or to get his recollections on the issues of his years as dean, but we can hear Dr. Hubbard through his former students, Drs. Craig, Johns, Rapport, and other classmates who have turned out pretty well. Their origin stories certainly place strong emphasis on the roles of the University of Michigan Medical School, deans like Hubbard, and many of the Medical School teachers who helped form generations of leaders and best.
Postscript.

Clair Cox was one of the leaders and best to have come from the University of Michigan Medical School. As a resident in the 1970s at UCLA, reading the urology literature, I became familiar with the name Clair Edward Cox, II, who published interesting and good papers from Bowman Gray School of Medicine (now Wake Forest Medical School) and later the University of Tennessee in Memphis. Little did I know we would become friends during my time in Ann Arbor, where the University of Michigan connected us. I’m sad to report that Clair passed away a few weeks ago.
Clair was born on September 3, 1933 in St. Francisville, IL, and grew up in Mt. Pleasant, MI, excelling in studies and sports. With a Regents Alumni Scholarship, he completed three years of undergraduate studies at the University of Michigan and then entered the Medical School. In his sophomore year, he met junior nursing student Clarice Adele Wicks and they married in 1958 when Clair graduated with an M.D. His Medical School Class of 1958 was a remarkable group in a remarkable time, entering postgraduate medical education in the new era of specialty practice, massive research funding, and a high point of academic medicine. At Michigan, this was at the end of Furstenberg’s long tenure as dean, from 1935 to 1959, when the dean practiced medicine at nearly a fulltime clip whilst tending to the medical school administration. Frederick Coller retired as chief of surgery in Clair’s graduating year and Reed Nesbit, head of urology, was nearing the peak of his career having brought Transurethral Resection of the Prostate (TURP) to the mainstream of international urologic practice. Both men inspired Clair as a medical student and Nesbit, particularly, became a resource as Clair ascended the hierarchy of academic urology.
Clair and Clarice moved to Denver for surgical training at the University of Colorado, anticipating a path to thoracic surgery, but urology gained the upper hand in his interest and the couple continued west to San Francisco for urology training that he completed in 1963 at the University of California. The couple returned east across the country to Winston-Salem, NC for an academic urology position at Bowman Gray where Clair advanced through the ranks to professor. In 1972 Clair was recruited to lead urology in Memphis at the University of Tennessee and held the chair position for 27 years until he stepped down, having trained 90 residents. He continued to work for another 10 years until retiring in 2009.
Dr. and Mrs. Cox raised four boys who would give them 12 grandchildren. In retirement Clair enjoyed his family, their home, and the family ranch in Hernando, Mississippi. His last academic paper, a historical investigation, entwined the stories of a fellow Memphis urologist (Thomas Moore), Graceland, Elvis Presley, and the American Urological Association. Michigan Football frequently brought Clair, Clarice, and occasionally a son and grandson back to Ann Arbor. Of Clair’s multiple university affiliations, the Michigan connection was the strongest, as evident to visitors to the lovely Cox home on Sweetbriar Cove in Memphis where maize and blue colors and UM symbols flourished. The Nesbit Alumni Society includes UM Medical School graduates along with the UM trainees who became urologists and Clair was pleased to be a member, after all Nesbit was his first teacher of urology. Clair once said that while he enjoyed working in five excellent medical centers, it was the University of Michigan that was always closest to his heart and running through his veins. Just as he felt the University of Michigan distinguished him as a citizen and a urologist, he distinguished the University of Michigan as an exceptional alumnus, educator, clinician, and scholar.
Clair Edward Cox, II, died peacefully at home on July 9, 2020. [Above, Dr. Cox on his ranch in Hernando, 2017.]
Thanks for reading Matula Thoughts, this first Friday of August 2020.
David A. Bloom
University of Michigan Department of Urology