Matula Thoughts May 1, 2015
2992 words
Some recent readers of these essays, Matula Thoughts, have asked what it’s all about. For a little more than 15 years I’ve been putting out a mixed bag of observations as a monthly e-mail communication, initially to the entire medical school faculty when I worked in the dean’s office of Allen Lichter. We called the communication What’s New, and I kept it going (expanded to a weekly email) after my fulltime return to the Urology Department. Currently, on most weeks What’s New is written by members of our department under Associate Chair John Wei as the primary author/editor, leaving me only with the monthly “first Friday” issue covering topics as diverse as Hippocrates, astronomy, healthcare, urology, etc. A little over two years ago, we spliced the first Friday issue to a parallel version on a blog called matulathoughts.org, explaining the title in an introductory piece on March 26, 2013. If you missed the explanation you can find it added to this communication as a post-script.
MH 26392)
1.  May’s long stretches of daily sunlight, entices us that summer is just around the corner. Claude Monet’s painting Woman in a Garden of 1867 (at the Hermitage Museum in St. Petersburg) shows one of those days that we’ve longed for throughout this long winter. A brush of snow last week challenged us briefly, but today the buds are on the trees, songbirds are in the air, and the hosta poked out of the ground for a few days until our local deer chomped them down. In May we drive home from work when it is still light outside. Whereas the USA celebrates Labor Day in the autumn, for most other nations May 1 is International Workers’ Day, an event that began around this time of year to honor workers according to an archaic view of the working class.
May’s long stretches of daily sunlight, entices us that summer is just around the corner. Claude Monet’s painting Woman in a Garden of 1867 (at the Hermitage Museum in St. Petersburg) shows one of those days that we’ve longed for throughout this long winter. A brush of snow last week challenged us briefly, but today the buds are on the trees, songbirds are in the air, and the hosta poked out of the ground for a few days until our local deer chomped them down. In May we drive home from work when it is still light outside. Whereas the USA celebrates Labor Day in the autumn, for most other nations May 1 is International Workers’ Day, an event that began around this time of year to honor workers according to an archaic view of the working class.
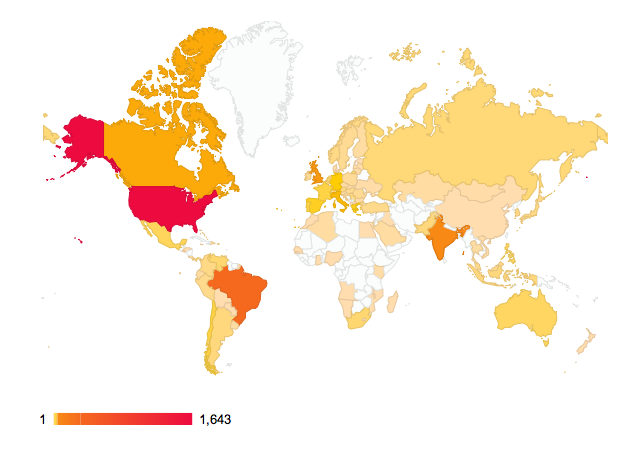
 [Source: Wikipedia. Dark blue = Labor Day on May 1, Light blue = another public holiday on May 1, Pink = Labor Day on another date, Red = No Labor Day]
[Source: Wikipedia. Dark blue = Labor Day on May 1, Light blue = another public holiday on May 1, Pink = Labor Day on another date, Red = No Labor Day]
Yet, well before those early public celebrations of the working class, Adam Smith and other thinkers were keenly aware of the division of labor, on which society depends so totally, into many specific jobs, trades, crafts, and formalized professions. Professions maintain standards of practice and systems of education, and the medical profession is one of the oldest. May happens to be a traditional time for medical school graduation, a lovely ceremony marking the emergence of a new cohort of MDs. When the first class of medical students graduated in Ann Arbor in the mid-19th century they were deemed ready to enter the workplace as new doctors after 2 years of lectures that comprised their professional education. Since then medical school has grown to 4 years of study that also includes laboratory investigation, self-study, and clinical experience. Graduation, an esoteric labor day of a sort, now marks a transition to the career-defining stage of medical education, namely residency training, a phase lasting an additional 4-10 years. Many medical schools, including ours at the University of Michigan, include recitation of the Hippocratic Oath at graduation to connect the graduates, as well as the established physicians present, to the ancient and durable principles of their profession.
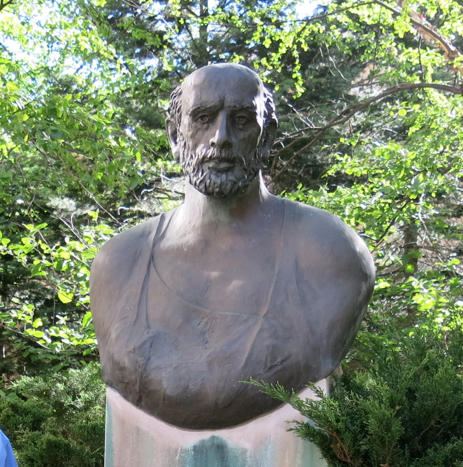

[Left: Hippocrates’ statue at UM. Right: UMMS graduates in 2013 who entered urology programs. Now, nearly PGY3s, they are halfway through residency. Sarah Hecht now at Portland, Nirmish Singla in Dallas, Adam Gadzinski in San Francisco, and John Delancey in Chicago at Northwestern]
2. This May is also noteworthy for the AUA Annual meeting when our faculty and residents present their work in the intellectual marketplace of international urology. Michigan urology usually has well over 100 podium presentations, posters, and other prime time appearances. The national meeting is the place to hear new ideas, discover new technologies, extend our reputation, spot new talent for recruiting, as well as reconnect with our own alumni and friends. Sunday’s Reed Nesbit Reception hosts well over 100 of our alumni and friends annually, and we will report on this next month. What does the Hippocratic oath have in common with the AUA? Both are manifestations of professionalism, the medical arts at large and urology in particular. Professions have a long record throughout human history, the medical ones going back to healer-priests, the Hippocratic School, and the Company of Barber-Surgeons as examples. In professions societies recognize the specialized knowledge of groups of individuals and accords them rights to practice, educate themselves, set standards, and innovate. These rights are conveyed in the interest of the public. It’s hard to imagine how government or the business world could perform these functions as well and as efficiently as do the professions in this day and age with 150 areas of medical and surgical areas of expertise, to say nothing of dentistry, pharmacy, nursing, podiatry, much less all the many other professions in the complex tree of knowledge. There is no free lunch, however, and the cost for these freedoms is a social contract in which the professions must look out for the public interest if they are to maintain the public’s trust.
3. The invisible hand that seems to maintain the efficient function of society is a useful metaphor that traces back to Adam Smith, if not before him. Some of that mysterious force is Darwinian and this is discussed nicely by David Sloan Wilson in a new book, Does Altruism Exist? Culture, Genes, and the Welfare of Others. He wrote: Group-level functional organization evolves primarily by natural selection between groups. This would explain evolution of the functional behavior of termite civilizations, bee colonies, and human society. The principle guiding hand in human society is hardly invisible and that is the hand of the ruling priest, king, or governing agency that sets laws and regulations to determine how people behave and how business enterprises work. A second factor, in addition to the regulatory laws, is at play in the commercial world and this is Adam Smith’s invisible guiding hand. Somehow the commercial world markets, largely and efficiently, regulate themselves. A third guiding hand comes from the professions, work groups that transcend mere jobs, to create cultures that set standards for their work, educate their successors, and fulfill expectations of the public. The profession of medicine has served human society from its earliest days and the Hippocratic Oath, dating back nearly 2500 years, is evidence of how a self-ordained profession can define its scope of work, declare its values, and pledge a set of behaviors in service to the public. Other professions have followed this model of an oath, although the Hippocratic remains the most durable and popular prototype.
4.  Rudyard Kipling is well known for stories and poetry, but I was surprised to learn he authored the Ritual of the Calling of an Engineer and that it was first recited as an oath at the University of Toronto 90 years ago today. The idea came from professor H.E.T. Haultain of that university, who believed graduating engineers should have an ethical framework. The Quebec Bridge disasters were a motivating factor and Haultain, on behalf of the Engineering Institute of Canada, persuaded Kipling to write the words. Other professions also grapple with ethical responsibilities. The American Institute of Architects recently considered a petition to consider whether its members should be censured for designing solitary-confinement cells or death chambers. An article by Michael Kimmelman considered the ethical issue of humane prison design: “What are the ethical boundaries for architecture? Architecture is one of the learned professions, like medicine or law. It requires a license, giving architects a monopoly over their practices, in return to a minimal promise that buildings won’t fall down.” [NYT. Critic’s Notebook. Feb 17, 2015. C1] The Institute rejected the petition, but the implication was clear that many members of the profession believe that the public deserves more than that minimalist promise of product stability. Codes of ethics and rituals bind people of like skills and interests together. Most professions derive their main value and meaning in relation to public service. It seems to be noble and virtuous for a profession to articulate and perpetuate its values and standards of service to the public. Ultimately, the professions exist at the pleasure of the public. When the public loses faith in the public service of a profession, that profession becomes just another business and a commodity. [Rudyard Kipling by Philip Burne-Jones. 1899. The Granger Collection NY. Public domain]
Rudyard Kipling is well known for stories and poetry, but I was surprised to learn he authored the Ritual of the Calling of an Engineer and that it was first recited as an oath at the University of Toronto 90 years ago today. The idea came from professor H.E.T. Haultain of that university, who believed graduating engineers should have an ethical framework. The Quebec Bridge disasters were a motivating factor and Haultain, on behalf of the Engineering Institute of Canada, persuaded Kipling to write the words. Other professions also grapple with ethical responsibilities. The American Institute of Architects recently considered a petition to consider whether its members should be censured for designing solitary-confinement cells or death chambers. An article by Michael Kimmelman considered the ethical issue of humane prison design: “What are the ethical boundaries for architecture? Architecture is one of the learned professions, like medicine or law. It requires a license, giving architects a monopoly over their practices, in return to a minimal promise that buildings won’t fall down.” [NYT. Critic’s Notebook. Feb 17, 2015. C1] The Institute rejected the petition, but the implication was clear that many members of the profession believe that the public deserves more than that minimalist promise of product stability. Codes of ethics and rituals bind people of like skills and interests together. Most professions derive their main value and meaning in relation to public service. It seems to be noble and virtuous for a profession to articulate and perpetuate its values and standards of service to the public. Ultimately, the professions exist at the pleasure of the public. When the public loses faith in the public service of a profession, that profession becomes just another business and a commodity. [Rudyard Kipling by Philip Burne-Jones. 1899. The Granger Collection NY. Public domain]
5. Scale. Our Department of Urology has reached a considerable size. When I joined the Section of Urology of the Department of Surgery, as it then was in 1984, I was the 6th faculty member and the only pediatric urologist. Now we have 5 pediatric urologists and a total of 37 regular faculty and 15 joint faculty shared with other departments. People ask: isn’t that too large a department? Or, how big should we be? The matter of size is important mainly from the point of understanding our mission and being able to execute it excellently. Our mission has three parts: education, research, and clinical care. However, from the mission derives our essential deliverable: kind and excellent patient-centered care, thoroughly integrated with education and innovation at all levels. This essential deliverable is both the milieu for deployment of our mission and our moral epicenter.
6. From the educational perspective, an excellent urology department needs to deliver great urologic care in all facets of urology. To teach urology a team of faculty needs to be engaged in urologic practice. This requires a certain depth of faculty, that is a redundancy of personnel to manage complex and routine urologic conditions around the clock. For some subspecialties in urology, such as andrology, two faculty members may permit ample coverage, whereas in other areas a larger number is necessary. For example, we hope to establish a program to provide 24/7 urinary tract stone coverage, whereby a patient can receive state of the art management of a stone by a full-time stone expert. This will require a team of at least 5 endo-stone urologists plus their support team. If it takes around 7000 RVUs to support one urologist, the clinical activity to support such a team can be calculated fairly quickly.
7. Another way to look at departmental size from the educational perspective is to consider the number of surgical cases necessary for a resident or fellow to become proficient at an operative procedure. The numbers vary among the facets of urology, whether pediatric urology, uro-oncology, pelvic-reconstructive urology, andrology or stone management. In the last example, we know that a minimum number of cases for a resident’s experience is 60 ureteroscopy cases, according to our certifying organization. The University of Michigan program of 4 residents a year for a 5-year training program, is organized such that those 60 cases are performed in the first two years of training, therefore we could calculate a need for a minimum of 120 ureteroscopy cases yearly. However, not all these cases are suitable for a novice, some cases will need to be performed mainly by faculty, and in many other instances a resident may not be available. Therefore it is no exaggeration to expect that a robust stone team should be performing at least 200-300 ureteroscopies per year. If it takes, let’s say, 5 clinic visits to generate one ureteroscopy, then a stone team might be expected to see at least 1000 – 1500 patients with stone disease a year. This type of back-of the envelope calculation could be extended to percutaneous nephrostomy cases, ESWL cases, or bladder stone patients.
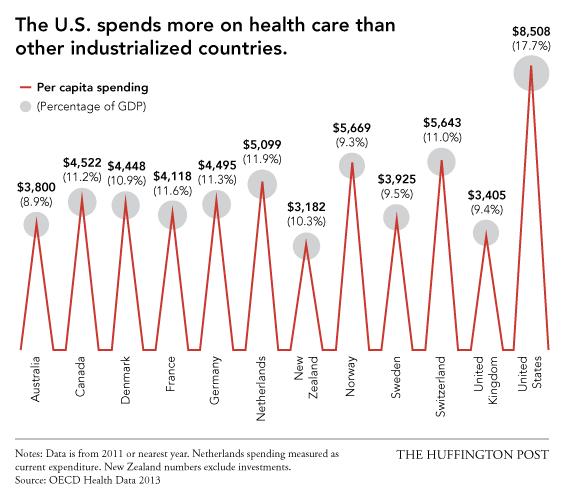
8. Yet another level of consideration of scale involves how many annual surgical cases are necessary to maintain proficiency. The average urologist in the United States performs less than 5 radical prostatectomies and less than 2 cystectomies annually. Because recent data (and common sense) correlates quality with volume, and it seems reasonable that a urologist who performs 30 cystectomies a year would be your preferred surgeon to someone who performs one a year, or one every other year. Thus a robust institution should deploy surgeons with robust volumes in their areas of expertise. The critical mass ensuing from a team of such surgeons, naturally would favor learning, teaching, and investigation worthy of a strong university. Decisions regarding size of an academic department are therefore most efficiently made within academia at the local level, recognizing that the history, geography, demography, economics, and politics of each institution, best determine its scale and destiny.
9.  Last month we mentioned Jack Lapides, Section Head of Urology here in Ann Arbor from 1968 – 83. Jack’s friend and contemporary Dick Lyon (seen second on your right and self-described as “old man.”) thereupon sent me this picture of Jack from 1975. In their era of practice a urologist was a generic general urologist. Few graduates of residency took fellowships, and most went out into practices that covered all aspects of urology. The world of urology has changed greatly since the days Lapides and Lyon, and considerable impact can be credited to their careers. Subspecialties have blossomed and Dick was one of the very first to identify with pediatric urology. Today it is most unusual in North America or Europe for a significant pediatric urology condition to be managed by anyone but a pediatric urologist, and this effect is diffusing throughout the rest of the world. A similar trend is forming for urologic oncology and neuropelvic reconstructive urology. The same subspecialization of labor is reflected throughout health care, other professions, and the workforce at large. This is an inevitable trend as knowledge accrues and technology expands.
Last month we mentioned Jack Lapides, Section Head of Urology here in Ann Arbor from 1968 – 83. Jack’s friend and contemporary Dick Lyon (seen second on your right and self-described as “old man.”) thereupon sent me this picture of Jack from 1975. In their era of practice a urologist was a generic general urologist. Few graduates of residency took fellowships, and most went out into practices that covered all aspects of urology. The world of urology has changed greatly since the days Lapides and Lyon, and considerable impact can be credited to their careers. Subspecialties have blossomed and Dick was one of the very first to identify with pediatric urology. Today it is most unusual in North America or Europe for a significant pediatric urology condition to be managed by anyone but a pediatric urologist, and this effect is diffusing throughout the rest of the world. A similar trend is forming for urologic oncology and neuropelvic reconstructive urology. The same subspecialization of labor is reflected throughout health care, other professions, and the workforce at large. This is an inevitable trend as knowledge accrues and technology expands.
10. While May Day historically celebrates the generic laborer, we recognized this is quaint terminology. Modern cosmopolitan life includes all sorts of workers of all sorts of skill levels. A myriad number of occupations not only contribute to modern civilization, they are the basis of it. Each skill and each job has dignity and should offer further opportunity. The great challenge for government, public policy scholars, and economists is to expand employment and mitigate poverty. All people deserve a chance for meaningful occupation and fair compensation. The most problematic divide in the world today is not between working class and an upper class, or between blue collar and white collar workers. The greatest divide is between the impoverished and the rest of mankind. Lacking viable jobs with sustainable wages that include health care and other benefits of a civilized society, an impoverished sector tends to perpetuate a cycle of poverty with all its attendant maladies. Its members are less likely to contribute to society, more likely to require substantial assistance, and their neighborhoods are more likely to explode, as evidenced this week in Baltimore. As we celebrate all workers in all the many specialized jobs of today, we should recognize the obligation to extend decent employment as widely as possible while maintaining a fair safety net for those left behind. This should be the promise of civilization.
 [Medieval Uroscopist]
[Medieval Uroscopist]
 [Garment Factory Workers 1936. Photo Russell Lee, public domain. The Living New Deal Website]
[Garment Factory Workers 1936. Photo Russell Lee, public domain. The Living New Deal Website]
 [WWII: FACTORY, 1942. Women installing an aircraft engine at the Douglas Aircraft plant in Long Beach, California. Photograph by Alfred T. Palmer, June 1942. Granger Academic]
[WWII: FACTORY, 1942. Women installing an aircraft engine at the Douglas Aircraft plant in Long Beach, California. Photograph by Alfred T. Palmer, June 1942. Granger Academic]
Post script (introduction from 2013)
Clues to predict the future have been highly prized throughout the millennia of human history, especially so when the future is related to prognosis of disease and disability. External cues from the heavens, in the weather, via tea leaves, or with playing cards have played major parts in the prediction of health. The logic of using more immediate evidence from physical signs or bodily fluids was evident to early practitioners of medical arts. Humans share the trait with other mammals of daily personal interest in their urine, for example, and its scrutiny during illness was obvious. Hippocratic writings documented uroscopy, as it came to be called, 2500 years ago and over the ensuing centuries the practice elicited imaginative prognostications as healers identified as uroscopists examined the gross characteristics of urine in flasks called matulas and speculated on the course of illness. The visual image of a “piss prophet” gazing at a matula served as the main symbol of physicians in art until only about 200 years ago when the stethoscope replaced the flask as medicine’s badge of office. We begin this electronic journal with a respectful tip of the matula to that original essayist Michel Eyquem de Montaigne who began his eclectic personal observations around 1572 when he was around 39 years of age. It is likely that Montaigne was well acquainted with physicians and matulas, as his father purportedly died of urinary stone disease and Montaigne himself began to suffer from them in 1578. What impulses compel us humans to share our observations and thoughts may someday be revealed through the matula’s diagnostic successors such as the MRI and other marvels of imagination, but there is no arguing that those impulses are strong and prevalent in our species. This blog (finally, I have used the awkward term) is a new forum for the monthly email broadcast I called “What’s New” that I started in 2007 in our Department of Urology at the University of Michigan and with the help of friends have continued regularly since then. These little spaces and sentences will be filled by things that a.) catch my attention and b.) I hope will interest some readers. For the most part this will be an alternative space and presentation of “What’s New.”
Best wishes, and thanks for spending time on “Matula Thoughts.”
David A. Bloom
v\:* {behavior:url(#default#VML);}
o\:* {behavior:url(#default#VML);}
w\:* {behavior:url(#default#VML);}
.shape {behavior:url(#default#VML);}
0
0
1
2820
16079
University of Michigan
133
37
18862
14.0
Normal
0
false
false
false
false
EN-US
JA
X-NONE
/* Style Definitions */
table.MsoNormalTable
{mso-style-name:”Table Normal”;
mso-tstyle-rowband-size:0;
mso-tstyle-colband-size:0;
mso-style-noshow:yes;
mso-style-priority:99;
mso-style-parent:””;
mso-padding-alt:0in 5.4pt 0in 5.4pt;
mso-para-margin:0in;
mso-para-margin-bottom:.0001pt;
mso-pagination:widow-orphan;
font-size:10.0pt;
font-family:Cambria;
mso-ascii-font-family:Cambria;
mso-ascii-theme-font:minor-latin;
mso-hansi-font-family:Cambria;
mso-hansi-theme-font:minor-latin;
mso-fareast-language:JA;}































 [Cholera & 1919 poster]
[Cholera & 1919 poster]
 [Yellow fever virus & vector Aedes aegypti]
[Yellow fever virus & vector Aedes aegypti]